How “Unprecedented” is the Kent Meningitis Outbreak?
Wes Streeting has expressed concern about the rapid spread and severity of the meningitis outbreak in Kent. According to UKHSA health officials, the number of confirmed cases has risen from 15 to 20. Streeting described the outbreak in Kent as “unprecedented”. Therefore, we thought we’d take a look at the data.
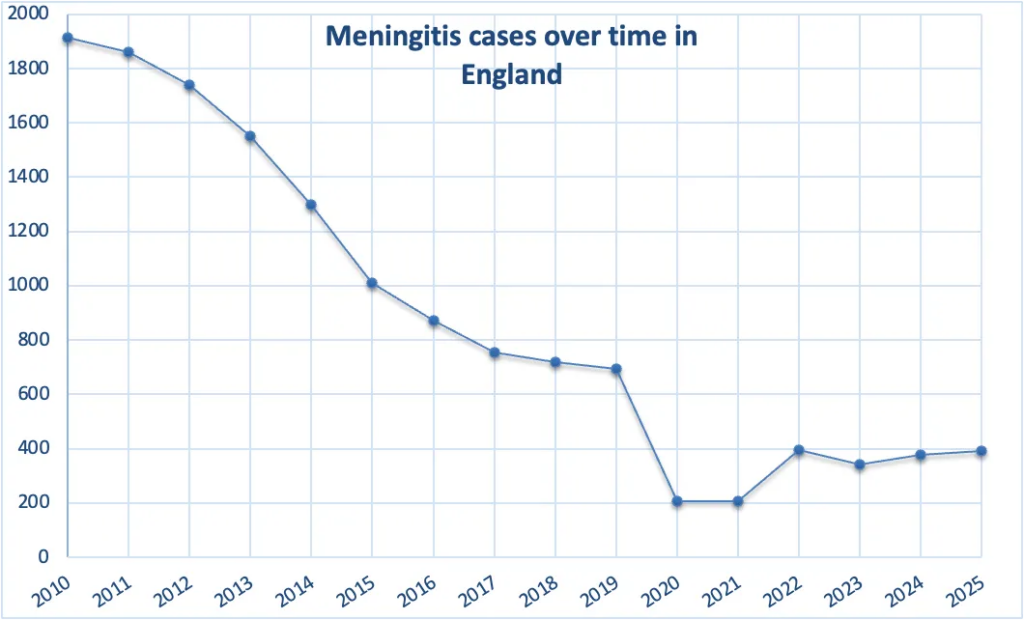
Based on UKHSA annual surveillance reports (2010-2025), the number of meningococcal cases in England decreased significantly, from approximately 1,915 in 2010 to 1,010 in 2015. This downward trend continued more gradually, reaching below 700 cases by 2019. In 2020, the number of cases dropped dramatically, largely due to COVID-19 restrictions. Following this decline, cases began to rise again, stabilising at roughly 340-400 per year.
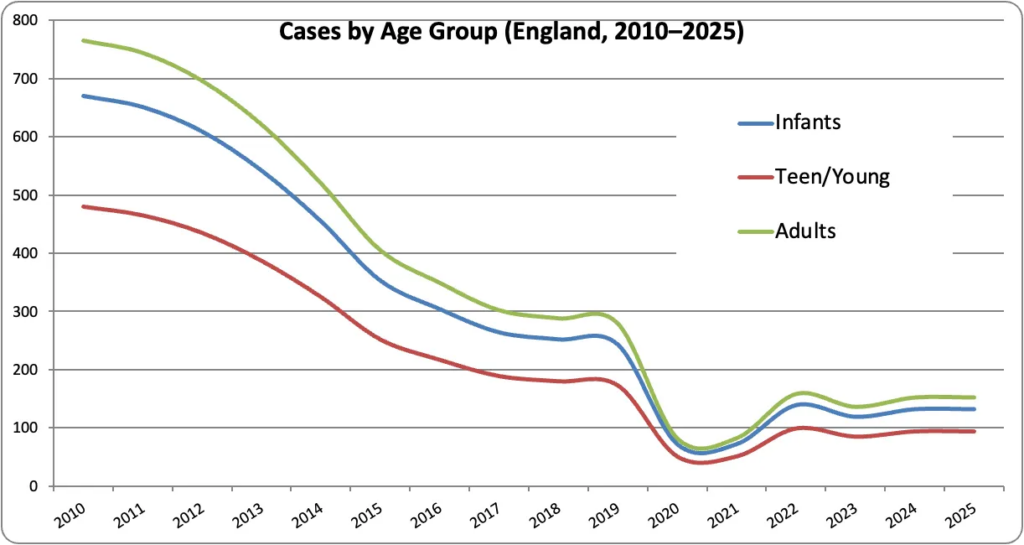
The case numbers for infants declined markedly from 2010 to 2019, dropped sharply in 2020, and then rose again post-pandemic. Teenagers and young adults formed the second-largest group, following a similar pattern of decline. Adult cases were lower overall but still showed the same temporal trend.
Across all age groups, cases decreased substantially over the decade, with a clear disruption in 2020 and partial recovery thereafter.
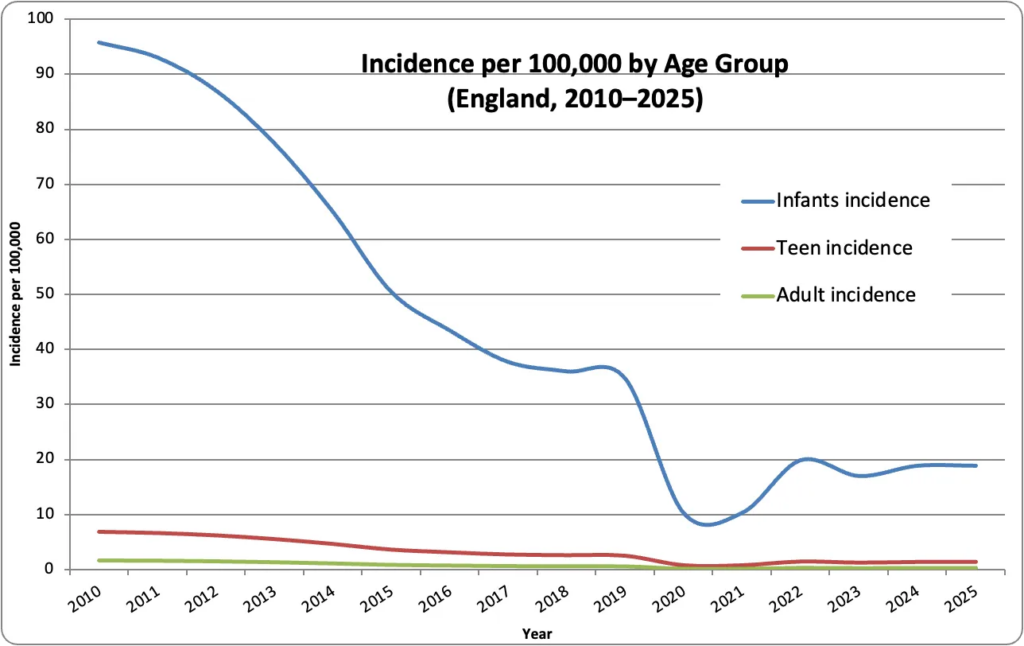
Making some assumptions about the age distribution of the population, infants have a roughly 15-60 times higher incidence than adults, who have a very low baseline risk.
Although overall UK meningitis incidence has fallen since 2010, there have been several notable outbreaks and clusters, mostly localised rather than nationwide epidemics.
Between 2015 and 2019, several UK universities, including Nottingham, Bristol and Edinburgh, reported localised clusters of meningococcal disease among students. These outbreaks were typically small but intense, often involving serogroups B or W, and were linked to close-contact environments such as halls of residence.
In 2015, students were urged to get vaccinated after a spike in meningitis cases. Figures reported 209 cases of MenW in 2015, with 22 linked deaths. The explicit warnings were targeted at students heading to university, who were considered a high-risk group. Liz Brown, chief executive of the charity Meningitis, said: “In the UK, every university could experience at least one case of meningitis amongst its students within the first term.”
Since COVID-19, the UK has not experienced large-scale meningitis outbreaks but has seen recurrent localised clusters, particularly among young people.
For example, a cluster of six cases was reported in the South of England in 2023, prompting targeted vaccination advice for students.
National surveillance data also show a rise in cases following the lifting of pandemic restrictions, reflecting renewed transmission rather than a single epidemic event. Public health warnings also highlighted increased risk among university students due to close-contact living environments. Together, this evidence indicates that meningitis remains endemic in the UK, characterised by repeated small clusters rather than widespread headline outbreaks.
The Kent 2026 meningitis outbreak differs from previous UK patterns in both scale and dynamics.
Earlier incidents were typically small, localised clusters — often involving five to 10 cases over several weeks — and were managed through routine public health responses such as contact tracing and prophylactic antibiotics.
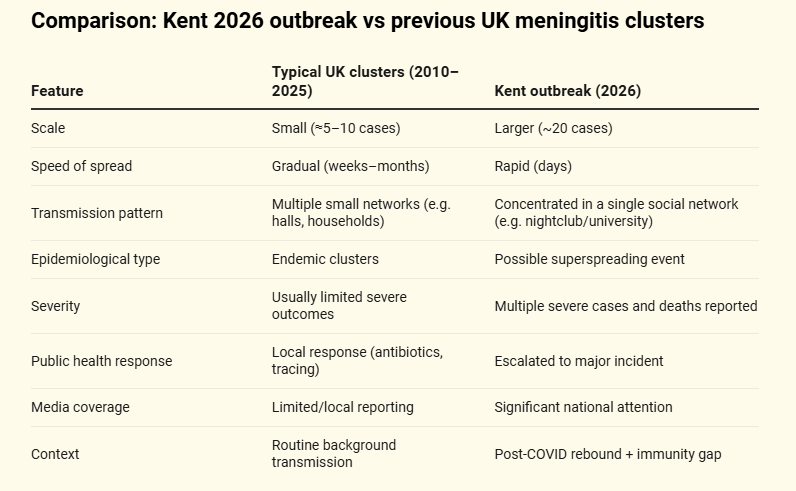
In contrast, the Kent outbreak involved around 20 cases within a very short timeframe and was linked to a single social network. At least 10 cases attended Club Chemistry in Canterbury on March 5th, 6th or 7th. It also resulted in multiple severe cases and two deaths, prompting escalation to a major public health incident. This contrasts with the usual endemic pattern of slower, contained transmission seen in the UK since 2010.
So, in answer to the question, the Kent outbreak is not unprecedented in the context of UK meningococcal disease, as localised clusters have occurred previously. However, it is unusual due to its rapid onset, relatively large number of cases within a single social network, and severity, distinguishing it from the typically smaller and slower-moving clusters observed in previous years.
This post was written by two old geezers who thought one of the functions of the UK Civil Service was to inform politicians before they made statements.
Dr Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack, Trust the Evidence, which you can subscribe to here.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Doesn’t the Civil Service regard its job as giving out incorrect information and biased politically motivated advice?
No. The civil ‘servants’ regard their job as stopping their minister achieving anything they disapprove of.
Imagine, if you will, that in club Chemistry certain recreational substances that have not been produced to the highest hygiene standards can be procured from some attendees…
Just imagination, of course.
Nah, according to Streeting it’ll be all about students “sharing vapes”. Because Streeting is on a Mission from God to destroy vaping.
Could have been worse. Imagine if it was Club Virology. Then we could all have fun watching Wes Streeting twisting his limited braincells sufficiently to convince us all that a “lab-leak hypothesis is (anti-Kent) Racist”.
Ahh. The Kent variant which became Alpha.
What is the likelihood this nasty strain of meningitis had its origin in a Russian or Chinese laboratory?
Firstly, meningitis and meningococcal disease are not the same which only adds to the confusion.
Secondly, no challenge study exists demonstrating human to human transmission of the disease. Instead a surrogate model (an apparently harmless bacteria) is used which (erroneously) assumes the pathogen already exists – this is a ‘begging the question’ fallacy. This is circular reasoning and circumvents the principles of the scientific method.
Thirdly, in these pseudo-scientific ‘infection studies’ participants are intranasally innoculated (i.e unnaturally exposed), observed, then it is assumed this ‘friendly’ bacteria will behave exactly as the pathogenic one. Again, this is not science, it’s another fallacy called affirming the consequent.
One cannot and should not infer with any confidence or authority from that which is not obtained using the scientific method. Doing so only exposes another fallacy, the false cause. This simply assumes, without proof, that a causal relationship exists between two events, overlooking other known factors that could explain the result (e.g recreational drug use/abuse, medications, environmental toxins etc).
You can replace ‘meningococcal disease’ with any named disease and the same outcome is observed. Because they have zero objective evidence, they simply circumvent logic instead.
Yes. Meningitis is inflammation of the meninges – the membranes around the central nervous system. It may be caused by a viral or a bacterial infection or by some poisons. Any vaccine would have to be specific for the virus or bacterium and would be irrelevant for a toxin. I’ve seen suggestions that these particular cases are bacterial. Bacterial infections take hold quickly and can play Hell with the body’s immune response. A comprehensive bacterial infection may not only inflame the meninges but also cause septicaemia (sepsis) leading to multiple organ failure. Nasty but not that unusual. In 2024 there were over 4,300 deaths due to sepsis in the UK.
There’s zero scientific proof bacteria or viruses cause meningitis symptoms.
The common belief that Neisseria meningitidis causes meningitis (or any other pathogenic microbes) is not a scientific fact, it’s pure fantasy because there’s no published experimental evidence.
Meningitis is a condition, not a specific infectious disease entity. It’s simply inflammation of certain tissues (meninges) … that’s it. English translations of papers from 1888 clearly expose the ‘false cause’ and ‘affirming the consequent’ fallacies. These frequently cited studies were not able to infer causation as they were only observational studies. Thus, only hypotheses could be generated as there was zero scientific evidence produced that demonstrated causation.
Those making the claim that bacteria/viruses etc cause disease must fulfil the following:
1) the cause microbes must be found in the diseased but not in the healthy
2)the microbe must be isolated from a diseased organism (human) and grown in pure culture
3)the save disease must be produced in a healthy host
4) re-isolation of microbe
To date, these logical postulates have never been fulfilled for any disease…not one!
If only Terrain Theory had won over showman Pasteur.
The whole edifice of Germ theory is the biggest con in human history.
Thank you Mr. Rockefeller/Carnegi, the Flexner Report. et al. Between you you’ve destroyed the halth of humanity.
And for those who believe their doctor – just do some research on the above.
100%
Big-pharma can’t make big money from terrain theory!
Thank you
That is very interesting and we also need to know what the hospital treatments given to the “cases” are. Not intravenous vit C no doubt.
I don’t suppose any of those who contracted the illness just happened to have been recently vaccinated and the strain of the contaminating virus just happens to be the same as the quackcine?
What a wonderful term: quackcine!
I had that thought, too.
What if they received some other vaccine in recent years that might have damaged their immune system.
I’m no medical expert but apparently for most people, this is like a case of the flu. We are told that there are 400 cases per year and the fatality rate is ten percent, but that’s just the reported cases, so how do we know, there may be a few thousand each year with meningitis who are tucked up in bed with a dose of paracetamol and lemsip who never know that it is not the flu. If that’s the case, then the death rate is considerably lower and we can panic a bit less and maybe the publicity around the current outbreak is causing more people to come forward and being diagnosed.
Love these two doctors and follow them religiously. I wonder why the UKHSA chose NOT to ask one of the UK’s leading expert infectious disease doctors to explain to the British public the facts regarding meningitis. Instead they threw Wes Streeting under a bus by making him, a non medical government employee, somehow to explain what was going on. Anyone else concerned about the poor response of this gov’t involving a deadly disease?
It’s to be hoped no one asks Sir Witless. I can imagine everyone, following the painted arrows on the ground, will be coerced into attending walk-in centres in car parks or the like to undergo a craniotomy…
Then again, a
stickswab pushed far enough up the nose with some degree of force could have a similar effect to cause harm.It’s not a “disease”.
It is the body ridding itself of toxin.
The vaccine manufacturers will be rubbing their hands with glee again at any proposition to increase sales.
I expect they will be re labelling the money pox jabs as we speak.
So often after reading the reported reaction of a government minister, my reaction is ‘I wonder what’s really going on’. Glad we have the two old geezers to help us work it out.
Well, fancy…. “Just months ago, in the last quarter of 2025, the government simulated a pandemic exercise, Exercise Pegasus, involving young people and a meningitis-like illness….” and part of it was coordinated by Kent and Medway Resilience Forum and Kent County Council…. what a coincidence!
(Thanks to Miri AF).
Interesting!
https://democracy.kent.gov.uk/documents/s134197/Exercise%20Pegasus%20Updating%20Report%20-%20Summary%20of%20Exercise.pdf
Oh there you go again using data and evidence to counter a good (repetitive) soundbite!
Dr Philip MacMillan reckons that the mild covid that was going around before this serious bacterial meningitis has caused a lowering of immunity in the sinuses. The covid virus causes interferon to reduce. Nitrous Oxide is blocked too and the bacteria, which can be present without causing symptoms, gets in and is deadly.
Nick Triggle from the BBC has, as usual, been trying to calm things down a bit, when the BBC headline-writers are doing all they can to scare us. Nick’s the only BBC journalist that I can remember providing anything like balanced reporting in 20/21.