“Carefully Reviewing the Data, the Chief Medical Officer Urged Calm”: What Our Covid Response Should Have Looked Like
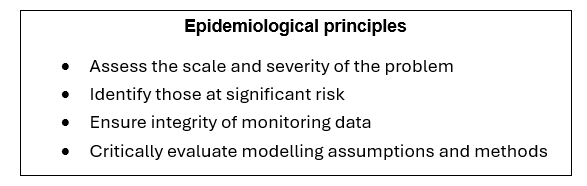
In a previous article we challenged the narrative that we hadn’t prepared for a pandemic. We then suggested that a set of core principles on how we should respond to future pandemics might provide a scientific, ethical and governance framework, and act as guard-rails, to help ensure responses are proportionate and appropriate in the future. Core principles could also potentially improve accountability of government advisors to politicians, and politicians to the public. We suggested principles under four headings: epidemiological, medical, ethical and democratic.
Here we attempt to describe how things might have worked out if we had applied them during the COVID-19 pandemic. After years of indoctrination with the standard Covid narrative many people might find it difficult to visualise how different it could have been – and many will not be old enough to have lived through earlier pandemics when we did manage them very differently.
So here’s an alternative approach to the COVID-19 pandemic, a traditional approach, using these core principles to respond to the actual data and evidence available at the time. We invite you to imagine a Chief Medical Officer (CMO) and a government committed to applying this framework of core principles to guide their decisions, starting at the beginning in early 2020.
Spring 2020 – The First Wave
In December 2019 reports of patients with a novel acute respiratory illness started to emerge from Wuhan in China. Mortality rates appeared to be high, 4.3% in one case series, and transmission to hospital staff and other patients common (41% of cases). Not surprisingly the CMO monitors this fast developing situation carefully, particularly the estimates of case fatality ratios (CFRs) that start to emerge from late January 2020, as shown below:
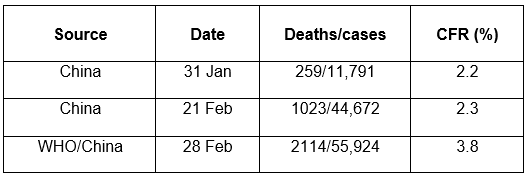
The earliest reports of CFRs from China were around 2.3%. Then the WHO/China Joint Mission identified more deaths and 10,000 more cases estimating the CFR at 3.8%. The CMO is aware that early estimates of CFRs for a new disease tend to over-estimate mortality, coming as they do from hospitals which only admit seriously ill people, and therefore missing in their count of cases those patients with milder disease in the community. What he really wants to know is the infection fatality ratio (IFR), that is the number of deaths from COVID-19 divided by all those infected, whether inside hospital or out in the community.
He therefore briefs the Prime Minister (PM) and Secretary of State for Health (SSfH) explaining that he expects IFR estimates will be considerably lower. He also shares with them the finer details from the February 21st report from China showing a steep age gradient and higher mortality in those with pre-existing conditions or co-morbidities, as shown below in Table 2:
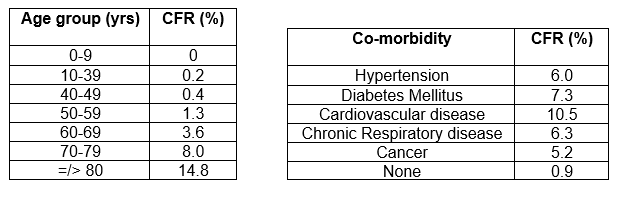
He emphasises that even in the oldest age group and those with cardiovascular disease, the large majority (85% and 90% respectively) survive an encounter with COVID-19, and that he expects these relatively high mortality rates to come down with IFR estimates.
In early March 2020 the CMO identifies two early IFR estimates and performs his own rough estimate of how the disease might affect the population of the UK, as shown in Table 3 below:
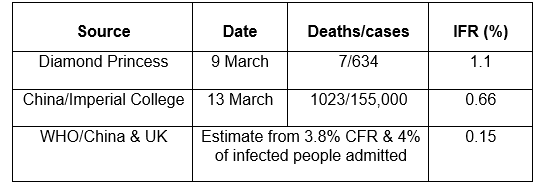
The Diamond Princess, a cruise ship quarantined in a Japanese port because of COVID-19 on board, identified seven deaths amongst 301 cases giving a CFR of 2.3%, the same as early Chinese estimates. However, continued widespread testing of the 3,711 passengers and staff on the Diamond Princess identified a further 328 people who had been infected and provided the first estimate of IFR at 1.1%, half of the CFR. The CMO is aware that this figure is likely to be higher than the UK as a whole would experience because of the older age of people on the cruise ship.
Next came an article from Imperial College which estimated the proportion of infected people in China from testing of returning ex-pats from China to Europe giving an IFR of 0.66%. Finally he derived an estimate of IFR using the highest Chinese CFR of 3.8% and a figure taken from the UK Pandemic Preparedness Strategy, which suggested 1-4% of patients with flu are likely to be admitted to hospital, and being cautious he used the upper limit of 4%. This suggested an IFR of 0.15%. He noted that even if 10% of patients with COVID-19 were to be admitted the IFR would still only be 0.38%.
So he concludes that the IFR is almost certainly below 1% and in his opinion nearer 0.5%. To put this another way he estimates that over 99% of people who develop COVID-19 will survive. Before briefing the PM and SSfH on these latest findings he estimates the IFR by age and co-morbidity using the figures in Table 2 and adjusting them assuming an overall IFRs of 0.5%, as follows:
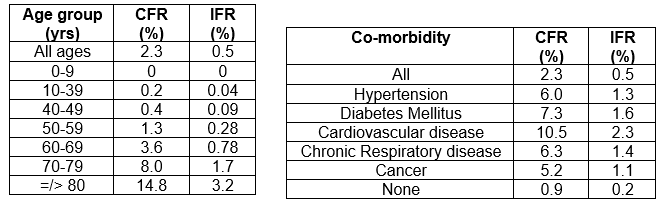
Unfortunately no cross-tabulation of age by co-morbidity was presented in the Chinese article to show, for example, the risk to those under 60 years with no co-morbidity, which he notes is likely to be significantly lower than the rates in table 4a, nor the risk to older people with multiple co-morbidities, likely to be higher than those in table 4a and 4b. Nevertheless, the CMO concludes that healthy people with no co-morbidity who are below 60 years of age are at a low risk from COVID-19. This view is supported by data from the first Instituto Superiore di Sanita report from Italy on March 20th 2020 as shown in Figure 1 below:
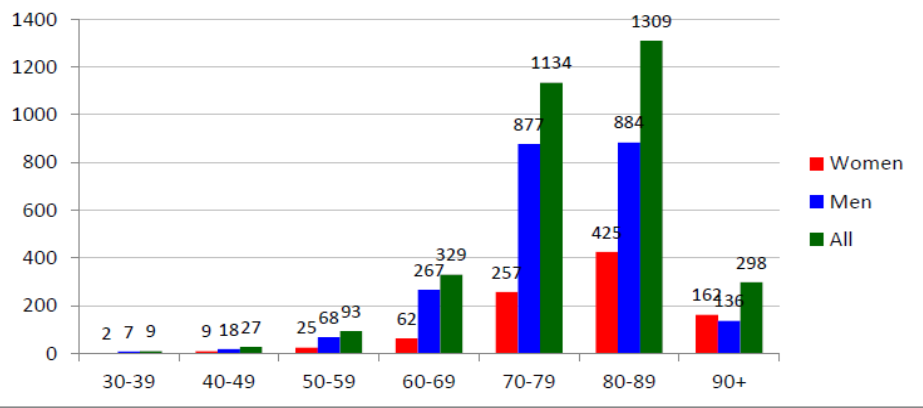
He notes once again that many of the deaths below 60 years of age in Italy would have occurred in those with co-morbidities, and also that men are at a higher risk than women. Finally he collates mortality data on previous pandemics for comparison:
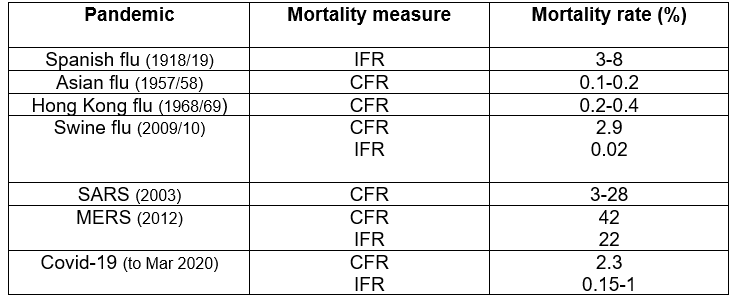
Although the comparison is bedevilled by not having IFRs on all pandemics it is still clear to the CMO that In terms of mortality COVID-19 with a CFR of 2.3% and an IFR of around 0.5% is no Spanish flu, SARS or MERS. and seems closer to Swine, Asian or Hong Kong flu. In terms of transmissibility it also seemed to him more like these previous flu pandemics than SARS or MERS, which fortunately were less transmissible. Furthermore he notes that, unlike these earlier flu pandemics, COVID-19 does not affect young people significantly.
The CMO discusses these data at a SAGE meeting where they also discuss the recent WHO/China Joint Mission report recommendations, and a modelling study from Imperial College which produced alarming results for some of its scenarios. There is a debate about the inconsistency of the WHO/China report’s recommendations in favour of highly restrictive measures to reduce the transmission of the virus on the one hand, with the equivocal evidence from systematic reviews from the Cochrane Collaboration and the WHO itself on the other. The debate about the Imperial modelling study is even longer because of the high numbers of deaths it suggests may occur, and the fact that demand for Intensive Care Unit (ICU) beds outstrips surge capacity in most of their scenarios. In view of some criticism in SAGE of the methods and assumptions in the Imperial study the CMO commissions a rapid critical review of it from a number of epidemiologists and statisticians working in the infectious disease field, whom he knows have a variety of views and perspectives. After a further SAGE meeting with the benefit of these reviews, recommendations are agreed and the CMO briefs the PM and Cabinet ministers.
Their recommendations are:
To reduce transmission:
- Isolation of cases – anyone with symptoms of COVID-19 to remain at home until symptom free.
- Household contacts of cases – monitor closely for symptoms of COVID-19 and isolate immediately if any develop, meanwhile work from home if possible and limit social contact to essential shopping etc.
- Standard ‘Catch it, Bin it, Kill it’ respiratory hygiene advice for everyone.
To protect the vulnerable:
- Advice to limit social contact for those 60 years and over and those under 60 years with co-morbidities for the next four weeks (shielding/focused protection)
- Healthy people below 60 years to continue as normal
To treat affected patients:
- PCR testing of patients with symptoms suggestive of COVID-19 in hospital only.
- Patients admitted to hospital with COVID-19 to be isolated from non-infected patients, healthcare staff to use standard PPE and face masks, and cohorting of nursing staff to minimise spread to other areas in hospital.
- Treatment with anti-viral drugs and antibiotics for secondary bacterial pneumonia plus symptomatic clinical support to be given to seriously ill patients.
No extension of COVID-19 testing beyond hospitals was advocated and no contact-tracing since it was clear the infection was already transmitting in the community. For similar reasons, no restrictions at UK borders were advised.
The recommendations were in line with the systematic review evidence with the addition of advice for vulnerable groups to ‘shield’. It was felt that this would protect these people until experience in treating COVID-19 improved or the virus mutated into a milder form, and would also help to reduce demand on NHS services so that they could maintain effective treatment of emergencies and urgent conditions like heart attacks and strokes. It was also recognised that continuing normal social contact amongst healthy people below 60 years would raise the levels of natural immunity in the population until the ‘herd immunity’ threshold was reached when viral transmission would be curtailed, further protecting vulnerable groups.
The commissioned reviews of the Imperial study were critical of some of their methods and assumptions and therefore said that their model outputs were unreliable. Nevertheless, the recommendations agreed went beyond the study authors’ maximum mitigation scenario which was estimated to reduce ICU bed demand by 70% and deaths by 50%. However, they did not go as far as the authors’ suppression scenarios which were attempting to stop viral transmission, in large part because of the certainty of causing extremely damaging effects across the whole of society.
Finally, to ensure accurate monitoring of the unfolding pandemic the CMO agreed with colleagues the use of the standard definition for confirmed COVID-19 cases, that is someone with relevant symptoms plus a positive PCR test. Data on hospitalisations caused because of COVID-19 were also to be separately identified from those in hospital for other reasons but testing positive, with or without symptoms of COVID-19. Finally, mortality data would record deaths where the underlying cause was thought to be COVID-19 separately from those where it may have been a contributory factor only and those where a positive PCR test was an incidental finding.
With these key decisions and actions the CMO and SAGE had applied the core epidemiological principles and recommended an appropriate and proportionate response to the early pandemic.
The CMO then briefed the Cabinet and in turn the government briefed Parliament, where there was a full discussion and some challenge because we were taking a different line to many countries, but the measures were eventually supported and implemented. The PM and CMO briefed the nation and press on the IFRs, how they varied by age, sex and co-morbidity, and on the recommendations.
Summer 2020 – The First Trough
During late March and April the NHS had become busy with an increase in medical admissions from COVID-19, but had managed to cope with the extra ICU capacity created and in some hospitals curtailment of elective surgery for a few weeks. Primary care had also been busier than usual but had coped. Now moving towards the summer, COVID-19 admissions were falling and services getting back to normal. The first wave was over and it was already clear that there was a strong seasonal effect to the COVID-19 pandemic, as expected.
Meanwhile further evidence on the COVID-19 IFR had emerged. A seroprevalence study, where the proportion of people infected is based on measurement of antibodies in the blood to SARS-CoV-2, was reported from Santa Clara county in California at the end of April 2020. The authors estimated that 54,000 people had been infected at the time when known COVID-19 cases were only 1,000 and deaths 94. This gives a CFR of 9.4% and an IFR of 0.17%. Then in early May Iceland, which had conducted PCR testing more widely than any other country, identified 10 COVID-19 deaths, 1,798 cases and estimated that there was 3,640 infected citizens suggesting a CFR of 0.56% and IFR of 0.3%. These further details were reassuring, suggesting that the CMO’s estimate of 0.5% may have been a little high.
With lower levels of virus circulating in the summer, government advice to vulnerable groups on shielding was updated with a recommendation to balance the lower risk of catching COVID-19 with the still serious nature of the illness on the one hand, and on the other how much they wanted to return to their usual social activities. This encouraged individual informed decision making and resisted the temptation to infantilise the population. All other recommended measures remained.
A number of pharmaceutical companies had begun trials of vaccines for COVID-19 in the early summer, offering the possibility of further protection for vulnerable people in the future. After discussion within the medical profession across a number of countries, other trials were being set up to test early treatment protocols. These were based upon the observed pathophysiology of COVID-19 infections using anti-viral, anti-inflammatory and anti-coagulant drugs, including so-called re-purposed drugs with well-known safety profiles. Finally, trials examining the effectiveness of vitamin D in COVID-19 were started based upon epidemiological and clinical research suggesting that deficiency increased the severity of respiratory infections and plausible physiological and immunological mechanisms.
Autumn/winter 2020 – The Second Wave
As expected, COVID-19 cases in the community and hospital admissions started to tick up in the autumn of 2020. The government and its advisors carefully considered whether any change to their first COVID-19 wave recommendations were needed.
Over the summer the CMO and SAGE had continued to monitor the progress of the various studies on vaccines, treatment protocols and vitamin D. They had also reviewed a large body of wider evidence on vitamin D and COVID-19, and viral and respiratory infections more generally. They concluded that the risk factors for Vitamin D deficiency and severe COVID-19 matched closely, that evidence for deficiency correlating with poorer COVID-19 outcomes was convincing, and that there was extremely strong evidence of widespread deficiency in the UK population. Furthermore, there was good evidence that vitamin D supplementation reduced respiratory infections. There was also evidence of other health benefits by correcting deficiency and minimal side effects, toxicity only occurring at extremely high levels of supplementation given over prolonged periods. Even though the vitamin D trials for COVID-19 were still running, given the above evidence and support for population level supplementation in the scientific and medical communities, they decided to recommend vulnerable groups to take 2000IU or 50mcg per day.
Preliminary results from the treatment protocol trials were showing improved outcomes with many already achieving statistically significant results, with only mild and rare side effects. Whilst the trials were continuing the CMO and SAGE decided to recommend their use in vulnerable groups in the community to prevent clinical deterioration and the need for hospital care, with a clear explanation to patients of the current strong but inconclusive evidence so they could make an informed decision.
Early results were also emerging from the vaccine trials showing that the number of symptomatic COVID-19 cases was significantly lower in vaccinated individuals compared to the unvaccinated. Relative risk reductions of COVID-19 cases in the trials sounded impressive at 70-95% but absolute risk reductions were only 1-2%. Some side-effects had been noted in the trials, most appeared to be mild and self-limiting but some were of a more serious nature. Despite having insufficient data on vaccine effects on severe disease or mortality the pharmaceutical companies were wanting to halt the trials and ask regulators for approval to market their products. The Medicines and Healthcare products Regulatory Agency (MHRA) reviewed the situation and discussed it with its counterparts in the USA and Europe. The MHRA was particularly mindful of the lessons learned from its approval of a new vaccine, Pandemrix, for Swine Flu in 2009. This vaccine had to be withdrawn because of unacceptable levels of serious neurological side-effects. The three regulators eventually agreed that the trials should proceed to collect sufficient data to determine the vaccine effects on severe disease and mortality and to better document types and levels of side-effects. They therefore refused approval for marketing and use of the vaccines at this point. They also stated that emergency or temporary use authorisation was inappropriate with a new gene-based technology with limited information on biodistribution and longevity of action, limited data on effectiveness and safety or toxicity to date, and with safe and effective alternative treatments becoming available.
Over the summer SAGE had also followed up reports from clinicians suggesting that there seemed to be a link between obesity and poorer COVID-19 outcomes. They noted plausible mechanisms and high-level observational data that supported this assertion, and a systematic review that confirmed poorer outcomes with obesity (increased hospitalisations, ICU admissions and deaths). After discussion with the CMO they added people with obesity to the list of vulnerable groups and agreed another specific recommendation.
So in autumn 2020 the authorities broadly reaffirmed their first wave recommendations, with some adjustments to the shielding one, and added three more:
To protect the vulnerable:
- Advice to avoid large social gatherings over the winter for those 60 years and over and those under 60 years with co-morbidities and obesity to minimise the risk of developing COVID-19 (partial shielding/focused protection)
- Daily vitamin D supplements of 2000IU (50mcg) are recommended for people 60 years and over, and those under 60 years with co-morbidities and obesity.
- People who are overweight and obese should reduce weight to lower their risk from COVID-19, as well as other health problems, and focus on reducing their carbohydrate intake.
To treat affected patients:
- Use of early treatment protocols in the community are recommended to prevent clinical deterioration (anti-virals, anti-inflammatories and anti-coagulants).
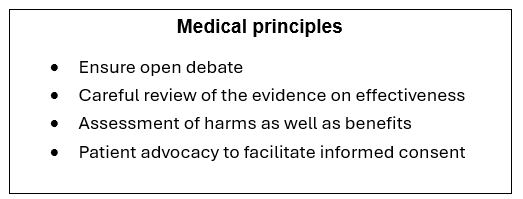
In their decisions leading up to the second wave UK advisors, regulators and the government had applied the medical principles in an open and transparent way:
And they had also upheld ethical principles around individual informed consent:
2021 and beyond
The early winter of 2020-21 proved to be busy for the NHS with COVID-19 cases in the community rising but with less pressure on beds than expected, perhaps because of vitamin D supplementation within the vulnerable groups and the widespread use of early treatment protocols. COVID-19 mortality and all cause excess mortality was also much lower than in the first wave. After Christmas, cases in the community started falling and it appeared as if the herd immunity threshold had been reached, controlling transmission of the virus.
An update on the IFR was published on January 1st 2021 by Ioannidis, when he reported on a systematic review of seroprevalence studies globally and concluded that 0.23% was the best estimate of IFR. Later in the year he reviewed all systematic reviews and in May 2021 produced an overall global estimate of 0.15%. Ioannidis’s findings were reassuring and confirmed the CMO’s assessment of the severity of COVID-19 in our fantasy UK pandemic response.
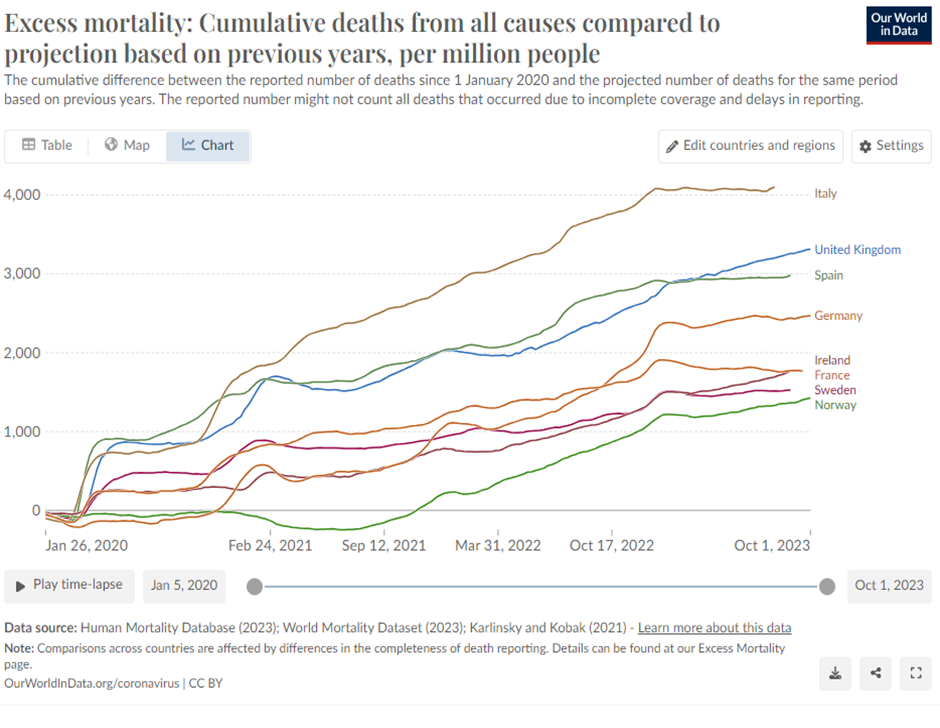
So what would have been the outcome if we had handled the pandemic in the way outlined? We can be certain that the damage to children’s education, the economy and society would have been far less; basic freedoms and quality of life would have been preserved; and we would have avoided many negative impacts on health, especially mental health, compared to a far more restrictive response. The impact on all-cause mortality is less certain, but it is likely it would have been closer to Sweden, the only country in Europe which did take a similar path to the one outlined here:
We are aware that huge pressures were brought to bear on all governments and their advisors for more restrictive measures throughout the whole pandemic period. These pressures came from multiple sources, but particularly the WHO, other countries copying the Chinese lockdown approach attempting to suppress the virus, and from the continual clamour and challenge from mainstream media to do more. The apocalyptic scenarios outlined in the Imperial College modelling study combined with the WHO/China Joint Mission report advocating these restrictive measures must have been particularly hard to resist. We have imagined a group of advisors and politicians whose thinking capacity was not overwhelmed by the psychological pressures they were repeatedly subjected to, and who upheld the democratic principles outlined in our earlier article, shown below:
Conclusions
There seems to have been two crucial decision points in the COVID-19 pandemic – firstly March 2020 and the decision to lockdown or not, and winter 2020-21 when vaccine trial results emerged. The pressures in March 2020 were outlined above. There would have been similar pressures, and some additional ones from the pharmaceutical industry, in winter 2020-21 for the MHRA to approve the COVID-19 vaccines and for the JCVI and the government to recommend them.
Much greater thought is needed about how such pressures can be resisted in the future. The framework of core principles outlined here and in our first article could be a starting point acting as a containing and guiding structure – with medical and scientific, ethical and governance guardrails. They also contain other helpful elements. An open debate within both the medical and scientific communities will generate alternative views and perspectives from experts able to be more dispassionate because they are not at the sharp end of decision-making. These debates, together with those in Cabinet and Parliament, ensure all important aspects have been considered before final decisions are taken. As a result, they also support and give confidence to those who have to make difficult decisions, and could help to prevent groupthink amongst advisers and ministers. Being open with the public, giving them accurate and timely information and treating them as adults, rather than sheep to be herded this way and that, also helps to share responsibility and locate it, appropriately, with each individual so that he or she can make his or her own decisions on social contacts and treatments.
Finally, we have three other observations. Firstly, the UK Pandemic Preparedness Strategy was a helpful document that would have steered us towards the approach outlined here if it had been used. Secondly, respiratory viral infections are often the way in which nature shuffles us off this mortal coil; we cannot prevent all such events and it is hubristic to think that we can. Instead the focus should be on dying with dignity with our family and friends around us. And lastly, it is easier to manage a pandemic with the benefit of both hindsight and absolute power.
Dr Alan Mordue is a retired consultant in public health medicine and Dr Greta Mushet is a retired consultant psychiatrist and psychotherapist.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
The message was largely “keep calm” to start with – then something changed.
Whatever changed was political, not medical.
“Advice to limit social contact for those 60 years and over” Sod off – I am 60 and you can shove your advice where the sun doesn’t shine. Postpone being alive, indefinitely? No thanks.
As for the “Pandemic blah blah blah” document being “useful” – sorry but I think I am done with “public health”. Starts off maybe with the best of intentions and ends up where we are now – the Pandemic Industry.
Plandemic.
Viruses don’t exist. Happy to argue with any who believe in the mythical beast.
Fake PCR cases mean nothing.
Patents on Rona stretching back 30 yrs.
Launched to prevent DJT winning in 2020.
Part of the US Military Corona Operation started in the 1960s – surveillance and spying.
But of course everyone knows that. Everyone is such a critical thinker.
It was indeed political. I remember that a certain senior politician went down with some kind of infection that was attributed to SARS-Cov-2 in one of the London hospitals. Someone (presumably an NHS worker) reported how heavy he was (can’t remember the number, but essentially he wasn’t very healthy). After that, he changed his mind and joined the panic club. You know the rest of it.
Lockdown started before Johnson “got covid”.
The Imperial modelling was the apparent trigger, but that is what we have been told publicly. We don’t know what was said behind closed doors.
The London cardiac arrest event (which I don’t necessarily think we can trust insofar as that or ANY data are concerned) kicked off when the U.S. said “15 days to slow the spread.” https://woodhouse76.com/2026/02/02/the-sound-of-sirens-new-york-city-and-london-spring-2020/ I’ve argued in multiple places that the phrase was the euphemistic activator of a military/intelligence-run drill initially pulled off in certain cities It’s most obvious in New York City, which was preceded by the [strategic] use of Lombardy (Bergamo especially, from a propaganda POV), and other staged “inciting incidents” beginning with Wuhan and proceeding to various “Patient 1s”, feigned outbreaks on ships and in nursing homes, etc. None of it would have been possible without social media and testing. [NYC overview here: https://woodhouse76.com/2024/12/16/new-york-city-spring-2020-an-unsubstantiated-mass-casualty-event-that-appears-fraudulent-and-staged/%5D We are still not at the point where those of us who contend that a pandemic was staged and that quantitative and qualitative evidence of various kinds show there was no sudden-spreading novel SARS-related virus causing a new disease on the scene in late 2019 or early 2020 are being acknowledged as having put forth very strong arguments. We are still too close to the event for the Overton Window to widen or shift beyond the bounds of false binaries which are limiting… Read more »
I am open minded. I’ve heard plausible evidence that something novel happened but lots of other plausible evidence to the contrary.
I like one of the last bits of the the second “false binary” piece – “Pandemics aren’t possible and preparing for them is a waste of time and resources”.
Like you we are not impressed by the recent performance of public health authorities.! In our articles we were wanting to emphasise that the government and their advisors had a responsibility to provide accurate and timely information to the public so they could gauge their individual level of risk. Then, with this information, individuals could make their own decisions on social contacts and treatments – informed consent in other words. So no mandates, no coercion, “advice” is simply that. “Sod off, I want to live my life” is one very understandable response, especially given what has happened, but the main point is everyone should be able to decide for themselves.
Thanks. Given where we are, the picture you paint is certainly preferable. It just doesn’t seem overly realistic and I have lost confidence that any public body can resist being corrupted despite best intentions.
Would certainly have been a big improvement on what actually did happen, but of course there are no certainties with a path not followed, so as mentioned the case of Sweden gives us our best most likely outcome. I don’t agree with the suggestion for PCR testing, as the Nobel prize winning inventor of PCR, Kary Mullis, consistently maintained it was not designed for, or intended to be a diagnostic tool. We knew from the experience of Italy what the profile of the illness was, if we assume for arguments sake there was actually a respiratory illness spreading. It was the old and the infirm, and recommendations (only) should have been made to those groups. Whatever we might think of the validity or otherwise of a viral illness called Covid-19, by the time it hit Italy our thoughts on the matter were irrelevant. What was not irrelevant, was the professional opinion of those who questioned the media led narrative. The use of HCQ and Ivermectin at known safe levels, with Decades of experience of these drugs, would have almost certainly have saved lives, from whatever cause by attenuating the presumed incidence of “cases”. Separating deaths from and deaths with, with… Read more »
I largely agree and you make good points about PCT and effective treatments.
While I believe that adults should be left to go to hell their own way, I have concerns about agencies of the state that purport to be and are seen to be authoritative (and are paid for by taxpayers) even advising people to stay at home or isolate or whatever. I think that only really applied to people who were already in extremely poor health. Most people over 60 that I know are pretty active and not a single
one that I know died of or with “Covid”.
This OAP worked out for himself six years ago the IFR of SARS-CoV-2 was likely roughly 100-fold less than the IFR of SARS-CoV-1 two decades earlier.
The Pandemic That Never Was became a self-fulfilling prophecy once the WHO branded it “SARS” (Severe Acute Respiratory Syndrome). Should instead have been called MARS (M for Marked).
Nowadays I’m inclined to agree that “Every single aspect of the ‘Covid’ narrative is fake. There was no pandemic…”
https://pandauncut.substack.com/p/every-single-aspect-of-the-covid
“…All the harms reported can be explained by a combination of:
a) Massive disruptions in health and social care: maltreatment, non-treatment or inappropriate treatment, especially of the infirm elderly
b) Misattribution of deaths to ‘Covid’
c) Other harms consequent to the response to the false perception that a novel deadly virus was circulating
d) Data fraud”
It was the State that Killed Granny.
I’m struck by the way the panic was coordinated across the world, from the video clips of people randomly falling over in China, to the insistence on masks that everyone acknowledged wouldn’t work… too much to be coincidental, the ‘response’ was planned and centralised.
Operation Corona – US military psyops started in the 1960s. Same name for the Corona Coup of 2019-20. Just a namecidence.
SARS-1 was also a farce, aided and abetted by a test co-developed by Christian Drosten, a chief architect on the WHO-endorsed 2019-nCoV (later SARS-CoV-2) test. If one reads the SARS-1 studies carefully, it’s obvious transmission and causality were not demonstrated. SARS-CoV-2 same.
As to self-fulfilling prophecy, I would put it this way: Given WHO-IHR criterion for declaring a PHEIC (precursor to pandemic declaration) “it” had to be a SARS-related virus (and was staged or “set up” to be such. https://woodhouse76.com/2025/08/06/does-a-sars-virus-automatically-trigger-a-who-public-health-emergency-of-international-concern-pheic/
Regarding the “social media reports” cited in the C-D test protocol, my bet is on the too-much-on-the-nose thread by Peter Danszak https://woodhouse76.com/2025/02/19/did-the-corman-drosten-protocol-rely-on-social-media-reports-to-seek-then-find-sars-cov-2/
That said, I doubt Herr Drosten, at least, actually did “first” hear about an alleged outbreak on social media.
Virologist Ron Fouchier said that he (Fouchier) heard in early December. Very possible that some (not all) of these scientists were fooled.
People such as Whitty, Hancock etc who ignored medical science and put us through all of that should be in jail on a charge of crimes against the UK public, and similar of course in the US, Canada, Europe and elsewhere. Why, why, why is the NHS still not loudly proclaiming benefits of Vit D etc.? You’d almost think that it suits our leaders for the NHS to be constantly at breaking point, but maybe I’m just being cynical!
It wasn’t about health – other than to try and maintain the illusion that “our wonderful NHS” is a competent, First World, system of delivering healthcare.
It was about CONTROL …… money, and accelerating The Great Reset.
A trenchant final papagraph. There’s a tale of an old-style hospital matron being heard to say, in response to having an embarrassment of elderly patients to look after, that a good bout of flu would be helpful to see them all off. Personally, I’d prefer that to a lingering death dribbling from all corners.
Fake PCR tests to inflate false positives. Fake Convid cases to scare the public and justify lockdowns followed by the Midazolam and Morphine cull of the elderly. Why are none of those reponsible for facilitating this scandal in prison??
Public health should only inform and advice.
That’s all folks!
“Public health” = the state = the last organisation I want advice from about anything, especially my health. They informed and advised me that various experimental, poorly tested medical products that were misleadingly labelled “vaccines” were safe, effective and necessary, and forced me to pay for them, and indemnify the manufacturers.
Before Covid, this is what PH did.
Not sure – I was not paying attention. They had been pushing vaccines for a long time, which some people think are bad for you/useless.
Only one word needed for Witless and Unbalanced – Sweden
This article is interesting, but it deals with the Covid pandemic as a purely medical incident. I think the majority of visitors to this site see the medical aspect as an excuse for governments worldwide to do something much more sinister. The control measures introduced by many regimes (not least our own) have done untold damage to mental health, education, society and the economy, some of which will never be undone.
My take on this is that the government panicked. Everywhere (except Sweden) instituted severe measures and if anywhere else had a pandemic protocol it was jettisoned, just as the UK one was. I believe that the government was scared that if they did not follow suit, and there was a catastrophe, they would be blamed for their inaction. They also relied on a worst case scenario which even at the beginning was clearly inaccurate. However there are a few things that might alter consideration of this narrative. First is the ongoing confusion between infection with SARS-CoV-2 and Covid-19. Covid-19 is a term that should be reserved for the serious but relatively uncommon consequence of SARS-CoV-2 infection, a cytokine storm. Covid-19 is identical to the cytokine storm caused by other triggers for which both diagnostic investigations and effective treatment were already in the public domain. There was, accordingly, no need for treatment trials which simply wasted months. People developing Covid-19 could be picked up by a diminishing blood oxygen saturation and specific blood tests. People with it required steroids and other immune modulators. Other cases of cytokine storm respond rapidly to these measures, as indeed the unnecessary trials confirmed. So, having… Read more »
Excellent article every medical student should read and learn not just the truth but also: “don’t listen to what your professors say but to what retired doctors say”