The Unsolved Mystery of How Viruses Spread – and Why Germ Theory Isn’t the Whole Answer
For over a century scientists have struggled to prove viral contagion. There are gaping holes in the current model of viral transmission but these holes are not a reason to throw out the concept of a virus. We need a new model that fits the evidence. Here I set out the evidence for and against the current model and suggest a way to reconcile the apparent contradictions.
Evidence for viral contagion
- Viral genetic material turns up in clusters of sick people. The sequences match. They change over time with new mutations in consistent ways without reverting. Even though testing is not perfect, people with positive tests are far more likely to be sick than not.
- Viruses have been well described. Even if isolation methods are not flawless, electron microscopy and crystallography have shown fine-grained details including the shape of structures like the surface of the spike protein.
- At high doses, transmission works. Human challenge trials demonstrate that viral exposure can cause illness when the dose is high enough.
- Genetic tracing of viruses during outbreaks shows that distinct lineages spread from person to person in predictable clusters, confirming person-to-person transmission.
This evidence explains the mechanism of viral infection. But it does not explain the timing of the waves of infection that are characteristic of many viruses like influenza and COVID-19.
Where the traditional model fails
- Normal-dose challenge trials often fail. The evidence here is strong: under experimental conditions, exposure frequently does not result in illness. A recent study confirmed this again.
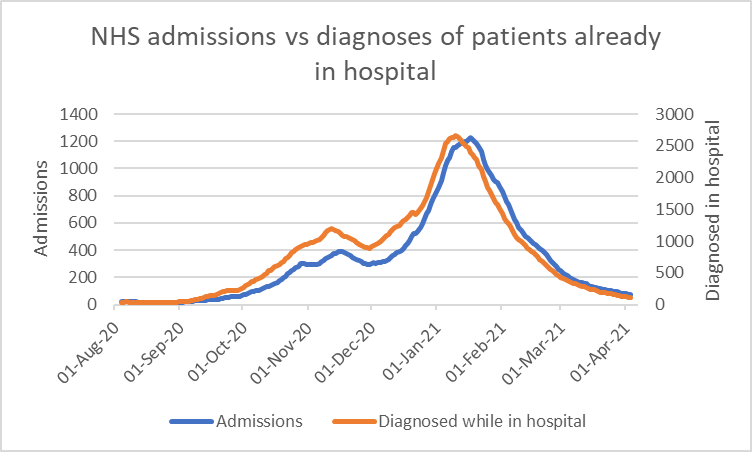
- Hospital-acquired infections peak at the same time as cases in the community. If spread were primarily driven by close contact, we would expect a lag, as community infections peak then admissions then within hospital infections. But the expected lag does not occur. In fact, hospital-acquired infections peak before the admissions to the hospital.
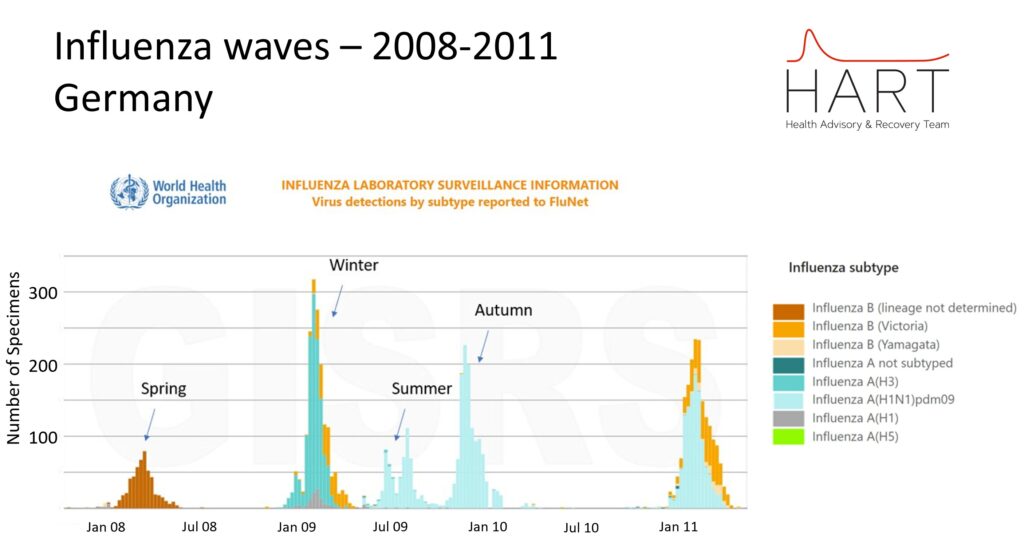
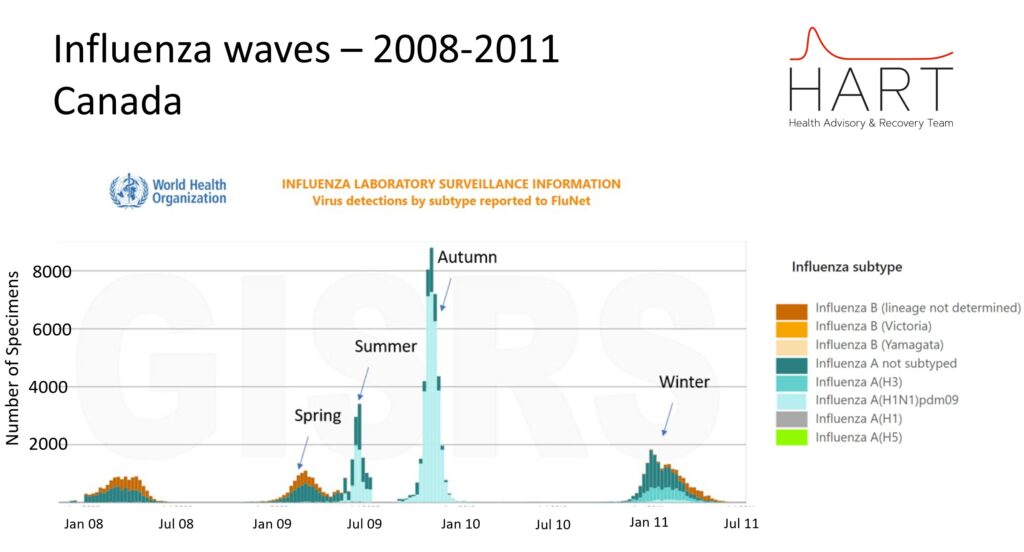
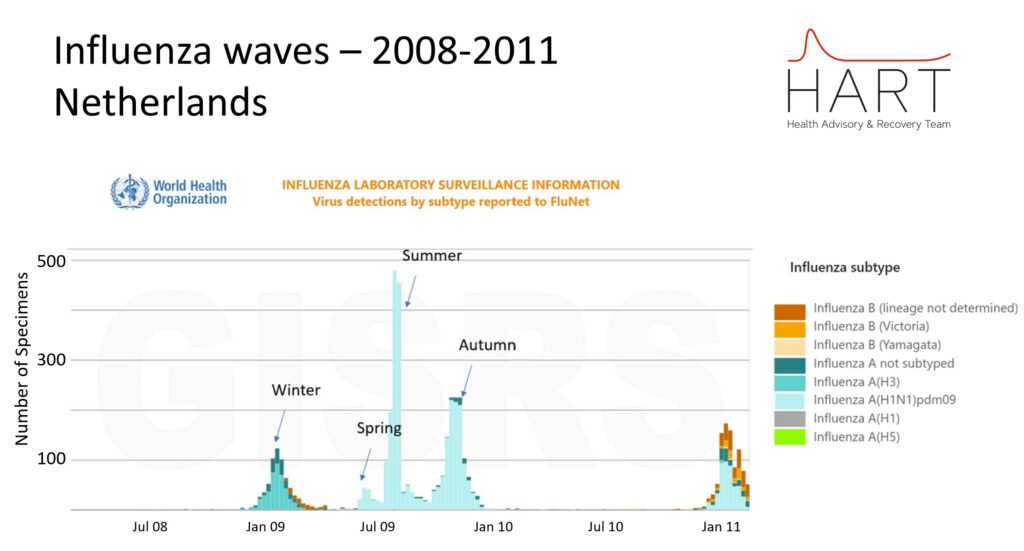
- Waves occur with seasonal regularity. Epidemic peaks in the UK often occur with peak deaths at predictable times of year before falling away for a time:
- Every early January
- Often early April
- Sometimes in July
- Every late October
In the USA, the southern states saw more of a summer wave during Covid and wastewater analysis for viral load shows a repeating pattern that continues to this day. The January 2022 Omicron wave (which occurred after a huge Christmas vaccine booster campaign) was exceptionally sharp in its rise and fall and followed by a deficit. However, the timing of peaks and troughs is predictable, with a low every spring and a peak every summer and winter.
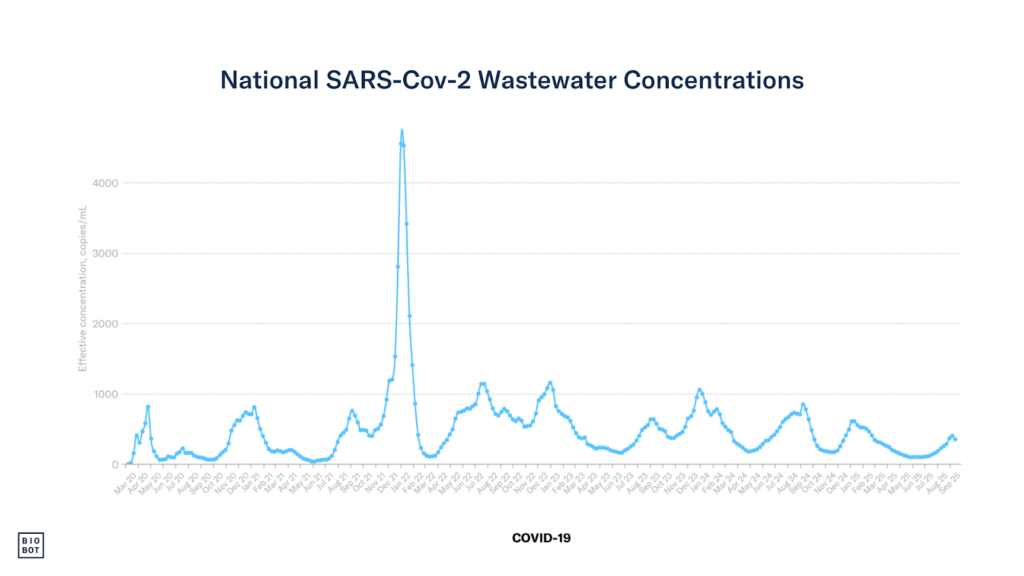
This is not explained by school terms or behavioural cycles alone. Lockdowns were a convincing (albeit unethical and very harmful) experiment that proved these things do not interrupt transmission. The steepness of the slopes and the timing of the peaks remained as would be predicted in the absence of lockdowns. The vaccinations did seem to impact the steepness of the January 2022 waves and the baseline levels of virus between waves from 2022, by increasing both.
The illusion of viral timing
It is often claimed that respiratory virus waves are driven by viral evolution or viral interference. In this view, waves happen when new variants arise that can evade existing immunity, which increases transmissibility and allows the virus to reinfect previously exposed populations. This idea has been central to the interpretation of influenza seasonality and SARS‑CoV‑2 waves, where ‘variants of concern’ with altered transmissibility or immune escape properties have dominated successive waves of infection worldwide.
If that were true, the pattern of waves should look a certain way:
- The spacing between waves would vary depending on when mutations appear or viruses outcompete each other.
- Some waves would be tightly packed, others widely spaced.
- There would be frequent overlaps of waves when mutations happened in quick succession
- Faster-mutating viruses would cause more frequent waves.
This is not what happens.
The reality is much more regular and much harder to explain by mutation or interference alone.
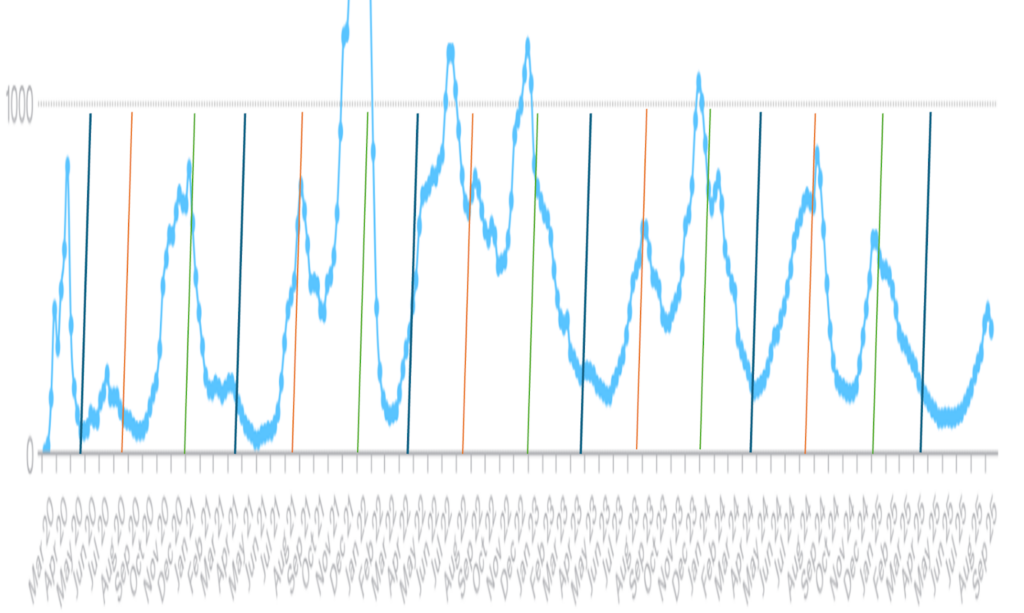
1. The timing is too consistent
In the UK and many other temperate countries, waves have arrived roughly every 13 weeks, across multiple years and virus types. This rhythm has held steady through variant shifts, travel restrictions and mass behavioural changes. Random events like mutation and competition do not produce this kind of precision.
2. Submariners are not protected from infections
According to the conventional virus-centric model, a respiratory virus wave ends when population-level immunity is achieved and subsequent waves occur only with new mutations. The rate at which mutations can occur in a closed environment will be a fraction of what can occur globally.
From this logic, we can infer what should happen in a sealed environment like a submarine.
- The crew is a closed, healthy population.
- Any circulating respiratory viruses will cause infections at the start of deployment.
- Once initial transmission occurs, everyone who is susceptible gets infected.
- The virus runs its course.
- The crew should then be universally immune to the strains that are aboard.
- No further illness should occur unless a new virus or variant is introduced.
But this is not what happens. The rate of acute respiratory infections was identical in submariners and those on the surface. In real-world submarine missions, respiratory infections remain common across the full duration of patrols. One study measured medical consultations from a centralised onboard medical system covering 240 submarine patrols lasting at least 10 days between 1997 and 2000, encompassing 13,441 male crew members (1,389 officers and 11,952 enlisted personnel) and over two million person-days at sea. Unlike for other illnesses, crew and officers and young and old had similar rates of respiratory illness. While they remarked on lower overall illness after 60 days at sea they did not claim there was any difference in the distribution of illness in this period. Unfortunately, they did not set out to measure this so we have no exact data, only the implication.
Despite minimal viral input and little opportunity for mutation or new exposure, new cases continue to arise. This directly undermines the idea that viral mutation is the rate-limiting step in transmission. New viruses and viral evolution are not driving these infections but changing host susceptibility may be.
Submariners are exposed to high levels of sewage derived bacteria which are maintained at constant levels in the air for weeks on end. These bacteria are detectable in the nasopharynx and in other circumstances are pathogenic and yet the rates of illness, both respiratory and gastrointestinal, remain as expected.
3. Faster mutation does not speed things up
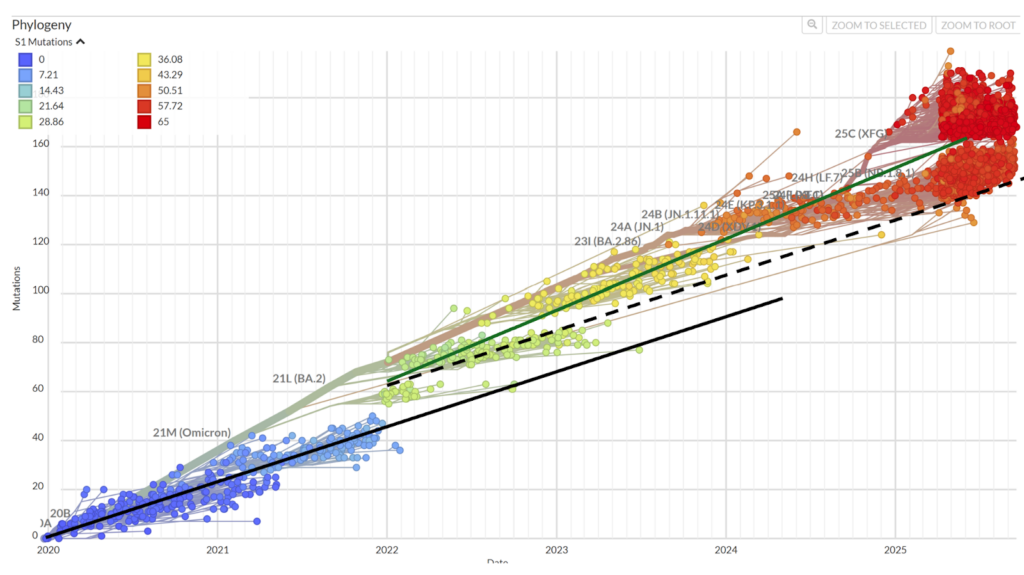
In the 24 months before December 2021, pre-Omicron SARS-CoV-2 accumulated around 20 mutations per year. From January 2022 to mid-2025, Omicron accumulated approximately 25 per year. Despite this 25% increase in mutation speed, the waves kept arriving on the same seasonal schedule.
4. Influenza mutates faster still and behaves the same
Influenza A mutates more rapidly than SARS-CoV-2, yet it too peaks once per season at a maximum. If mutation controlled wave timing, influenza should be constantly surging. But it too peaks at the same times of year as the slow to mutate SARS-CoV-2.
The trajectory of influenza and RSV is thought to look like this:
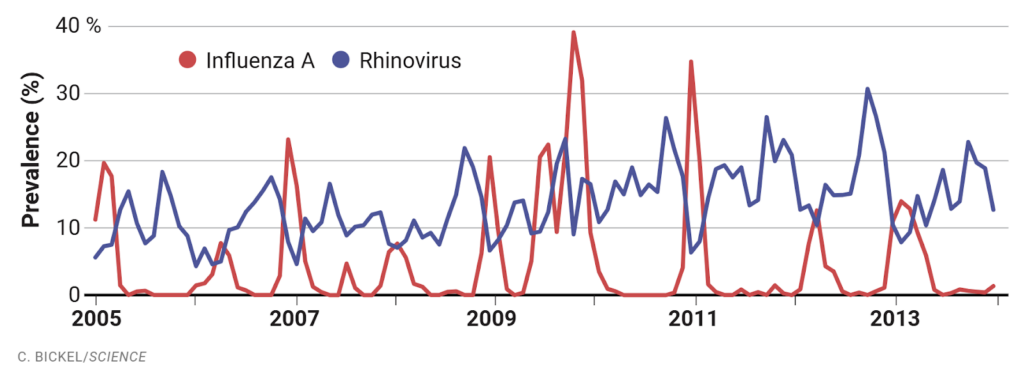
However, this prevalence estimate is based on testing of people who are sick enough to seek medical care and does not reflect the whole picture.
Conventional surveillance testing is focused on the sick and suggests that influenza only has a significant presence in autumn and winter. However, when testing is expanded to less sick people as happened in 2009 there is clear evidence of a peak in influenza each season.
Similarly, WHO’s global RSV surveillance strategy explicitly dropped the fever requirement for testing, recognising that around half of RSV cases, especially among children and the elderly, presented without fever and were systematically excluded from testing. While formal results are pending, the change reflects a recognition that traditional surveillance has masked the true scope and timing of RSV circulation.
5. Hospitals are full of virus aerosols year-round but infections still peak and fall
Air samples from hospitals consistently show SARS-CoV-2 present, even between waves. If exposure alone drove infection, we would expect ongoing hospital-acquired spread. But in-hospital infections rise and fall in synchrony with the community, including during troughs. The virus is still present in hospital air but the susceptibility is absent.
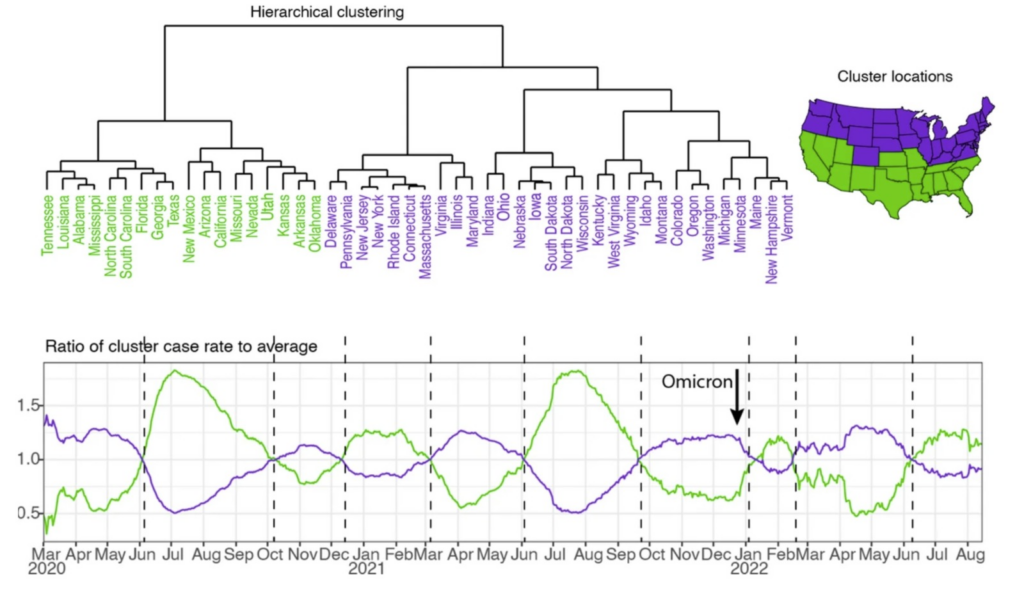
6. Spread skips regions
Each variant of SARS-CoV-2 spread country to country following the same seasonal susceptibility patterns as influenza. Large regions were skipped entirely in early waves e.g. Eastern Europe in spring 2020 and UK, Portugal, Ireland (i.e., the west of Western Europe) in spring 2021. If attack alone caused spread, this would not happen. But if susceptibility rises regionally, the virus already present in the air becomes dominant when the window opens. This would also explain why variants ‘spread globally’ at the same rate each time. Virus was also present in regions with no susceptibility and never took off, for example, all of South East Asia was not susceptible to Covid without any exceptions until all of South East Asia became susceptible without exceptions in early 2022.
7. Infections are determined by what is in the air at the time of susceptibility including coinfections
Often more than one respiratory virus is detected in an infection. So the idea that one virus has successfully outcompeted all others across a population does not hold up – if they cannot outcompete in an individual how could they in a population? When susceptibility rises, people inhale whatever is already in the air. That may be one virus or several. The virus that dominates is simply the one most widespread at that time and place.
We have seen this play out in ‘W-shaped‘ epidemic curves, where one virus briefly overtakes another mid-wave. Often these are sequential waves, but occasionally a Covid surge dips as influenza rises, or vice versa, then rebounds within one season. This shows that competition between viruses is real. But the overall wave, the rise, peak, and fall, stays on schedule. That means the wave is not being driven by the virus. It is being driven by susceptibility. The competition only shapes the subwaves of individual viruses inside it.
Why susceptibility fits better
If we assume viruses are circulating most of the time, but that illness only occurs when susceptibility rises in a portion of the population, then the pattern starts to make sense. The virus that dominates a wave is simply the one most prevalent in the air when that window opens. Regional synchrony, global emergence patterns and stable spacing between waves all follow logically from this.
Susceptibility explains:
- Why waves are regular
- Why whole regions can be skipped and hit later
- Why hospital infections synchronise with the community
- Why faster mutation does not change the tempo
Mutation and interference determine which virus dominates a wave but not when the wave arrives. Whatever is controlling when people get sick, it is not the virus.
The susceptibility model
The model that makes sense of these observations is one where infectious agents are necessary but not sufficient. The timing of illness must be due to something else.
There must be a third factor that:
- Peaks once each season (always in autumn and winter and not always in spring and summer)
- Affects only a fraction of the population each season
- Can spare certain regions entirely in any given wave
- Is capable of synchronising illness peaks across hospitals and communities
We do not know what this factor is but the data suggest it exists.
The evidence excludes certain possibilities:
- Human behavioural changes like school terms made no difference to peaks in lockdown.
- Temperature and humidity are important for viral stability, but do not have four seasonal peaks.
- Pollen, spores or volatile organic compounds do vary over the year, but not with the precision or global consistency needed.
- Other environmental factors like electromagnetic or space weather effects have cyclical differences but these track annually, not quarterly.
Any of these may play a role, but none independently explain the pattern. What might?
The immune clock
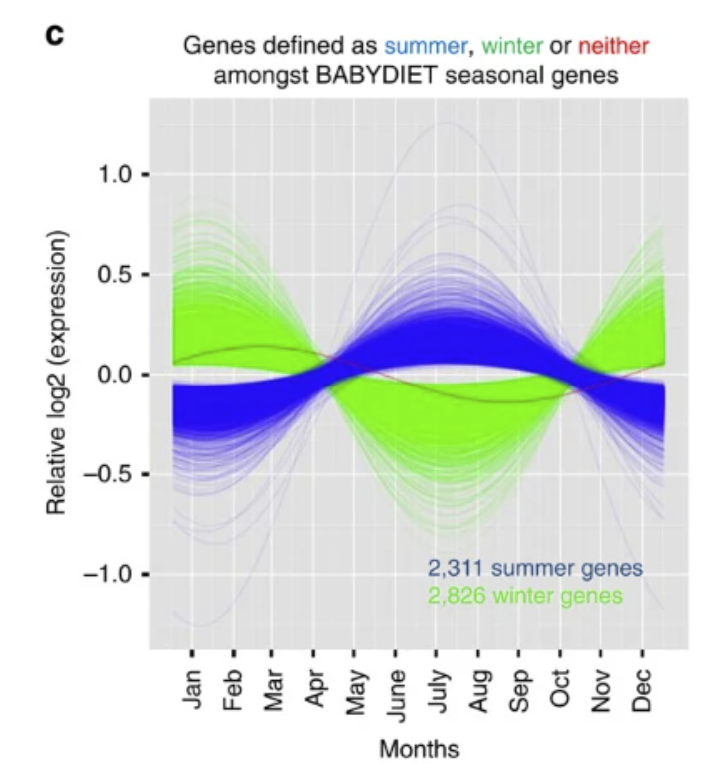
Our immune systems change with the seasons. Gene expression studies show clear and consistent shifts in immune pathways across the year – with January and July as polar opposites and transitional patterns in April and October. These changes are not subtle – nearly a quarter of genes are affected. The pattern is the opposite in Europe to Australia. In some cases, the winter and summer immune profiles are as different as those seen in entirely distinct disease states. These shifts in immunity profiles are reflected by changes to both the biome and susceptibility to pathogens e.g. COPD patients also show changes in their respiratory microbiome across different months of the year and influenza and coronavirus waves surge at predictable times as the immune profile shifts.
Susceptibility and dose
The two forces of viral dose and host susceptibility interact. In controlled human challenge trials, where viral doses are carefully administered and often far exceed natural exposures, symptomatic infection is induced in a higher proportion than seen in a natural wave. This shows that at high doses, exposure can overwhelm even a robust immune state, but that is the exception, not the rule. In real-world settings, exposure is often low from a few aerosols in the air, not a bolus of virus. In these low-dose exposures, host susceptibility becomes the dominant factor. If the immune system is in a defensive, resilient state, exposure may pass unnoticed. If susceptibility is high, due to seasonal, environmental or physiological factors, even a small viral input may be enough to trigger illness.
Whatever the factors are that lead to susceptibility they must overcome the mucus barrier of the respiratory tract which is normally impenetrable to viruses.
Is this hypothesis falsifiable?
There are three main explanations for the seasonal cycling seen in human immune gene expression:
- The viral mutation model. Immune cycling is downstream of viral exposure. Seasonal waves of infection, with everyone exposed to airborne viruses, drive immune activation, while gene expression shifts reflect that exposure.
- Innate biological rhythm. Each person’s immune system runs on a built‑in annual clock, independent of environment or exposure.
- Environmental entrainment. Immune function responds gradually to sustained environmental inputs – atmospheric, electro-magnetic or otherwise – which vary by season and location.
These explanations make different predictions. In particular, they differ in how quickly immune changes should appear when the environment or viral exposure changes.
If the rhythm is innate then nothing should change it. If immune cycling were primarily virus‑driven, then removal from seasonal viral exposure should produce rapid and marked immune changes. Conversely, if immune cycling reflects slow environmental entrainment, changes should accumulate gradually, with delayed recovery on return.
The fact that people in Australia have the opposite cycle of immune gene expression indicates that the rhythm is not innate.
The NASA twins study
The NASA Twins study provides a unique natural experiment. Astronaut Scott Kelly spent 340 days aboard the International Space Station (March 2015-March 2016), while his identical twin Mark remained on Earth as a control, exposed to normal seasonal cues and circulating viruses.
Scott was removed from Earth’s atmosphere, magnetic environment and from seasonal respiratory virus waves.
- Immune gene expression changes did not change immediately after launch.
- Instead, the number of differentially expressed genes was modest in the first six months and nearly six‑fold higher in months six to 12.
- On return to Earth in early March 2016, over 90% of gene expression changes reversed only slowly, over several months.
- 811 genes, including immune and DNA repair genes, remained altered six months after return.
If immune cycling were primarily a response to viral exposure, the most dramatic changes should have occurred early in the mission or early on return, when seasonal viral input was abruptly removed or replaced. They did not. The immune system did not react sharply either on entering space or on returning. Instead, immune modulation accumulated gradually, suggesting a lagged adaptation to a sustained environmental change, not a rapid response to missing pathogens. These observations argue against both an innate immune rhythm and virus exposure as the primary driver. They support a third explanation: environmental entrainment.
Further tests
This interpretation leads to specific, testable predictions:
- Astronauts or submariners returning to surface environments in different months would provide a natural test. If virus exposure alone were the key factor, immune markers should re-align with viral exposure with more rapid realignment during viral peaks. But if environmental entrainment is the dominant driver, then re-alignment would occur over weeks or months, regardless of viral exposure. Furthermore, testing for infections would demonstrate whether any infections were playing ‘catch up’ with viral waves that had passed in their absence or whether they were aligned with community infections.
- Antarctic researchers, overwintering in controlled environments with extreme photoperiod disruption, could help separate electro-magnetic exposures from microbial drivers.
- Passengers crossing hemispheres offer a natural test.
- Viral mutation theory says viruses travel from Australia towards Europe. If virus exposure drives illness, those flying north to south (e.g. UK to Australia) should be at higher risk than those flying south to north (e.g. Australia to UK), who’ve already been exposed. But if susceptibility is driven by environmental entrainment, there should be no difference: both groups would be equally vulnerable when immune profiles are misaligned with local conditions.
- Furthermore, infection risk should peak for travellers in January and July, when immune gene expression between hemispheres is maximally misaligned, and be lowest in April and October, when profiles naturally align temporarily. If illness follows this pattern, then susceptibility, not the direction of viral flow, is what governs risk.
Possibilities going forward
A complex web of interactions between multiple environmental variables might possibly help explain the phenomenon. Together, they might create a susceptibility environment that emerges on a roughly 13-week cycle, even if no single input has that pattern.
However, it could well be something we simply have not measured e.g. a seasonal atmospheric phenomenon that is invisible to our current tools.
It has been 170 years since germ theory was accepted. Scientific ideas evolve and this one needs to. The evidence shows that viral attack alone does not explain all the observations and a more nuanced model is urgently needed. If we want to predict and prevent illness, we need to stop staring only at the virus and start listening to the human immune clock and the environment it inhabits.
Dr Clare Craig is a diagnostic pathologist and Co-Chair of the HART group. She is the author of Expired – Covid the untold story and Spiked: A shot in the dark.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
No doubt the “virus deniers” that follow Lanka, Kaufman, Cowan, Bailey, Icke, Rappoport, Adams, Yeadon etc. etc. etc. will have something to say about that.
Good evening GHF. Many of us “virus sceptics” take exception to being called deniers.
I think that viruses exist, in so far as there exist particles of the size which virologists call viruses – for example exosomes. In some contexts it is useful to discuss things on this basis.
However the details of virology, as exemplified by Vincent Rancanielo (apologies if mis-spelt), just do not stand up to scrutiny.
From your list of the followed I commend Dr Mark Bailey for a concise, well reasoned and referenced paper ‘The end of virology’ which will at least raise doubts in any sceptical mind.
Both the Bailey’s are charlatans extracting money from the gullible.
Contagion depends on each individual’s immune system.
The existence of SARS-CoV-2 and all other viruses is beyond doubt.
Frank Visser, Steve Kirsch, “modern” virology and “whole” gene sequencing has blown the “viruses do not exist” argument out of the water.
Well, no, actually.
Please see my info re whole gene sequencing in my longer comment on the article. And if you are aware of any EVIDENCE of contagion please let me know. Virologists have spent many decades, carried out many experiments, to demonstrate contagion, but as far as I know none has succeeded.
Having no knowledge of whether viruses exist or not; it occurs to me that saying my experts are right and yours are wrong, is not a good argument.
just saying.
SARS-COV-2 never isolated. It was a creation of Drosten’s PC.
Porton Down in the 50s collected people willing to be infected with the cold virus.
None were.
Similar experiments at the end of Spanish Flu, which used direct attempts to spread the virus.
None worked.
Just saying…
I assume you are a medic?
Interesting debate. If susceptibility is seasonal as proposed, with the North and South hemispheres directly out of step, what happens at the Equator where daylight is relatively unaffected? Does susceptibility vary with latitude?
It does. This was brilliantly described by Edgar Hope-Simpson.
You can see the graphs he produced in this thread: https://x.com/ClareCraigPath/status/1604605792623251456?s=20
Unfortunately I do not use social media. But thanks to your reply I was able to find a ‘free pdf’ at https://link.springer.com/article/10.1186/1743-422X-5-29
Very interesting paper. Basically, vitamin D levels in the body define if you are likely to catch flu (and colds). This seems to work for me. In 2012 I caught 2 very unpleasant flu-like viruses, one in the winter and another in the summer (which I believe might have been caused by a tick bite). It occurred to me that I might be vitamin deficient so I started taking a vitamin drink every morning. Almost immediately I started to recover from the virus I had. I continued taking the drink and, during that time, did not catch a cold or flu for nearly 10 years afterwards even when everyone at work was catching colds. And I never caught Covid. I will let doctors argue about whether vitamin D has any effect, but since taking some vitamin D regularly is harmless, why doesn’t the NHS just give vitamin D to the elderly in the winter just in case it works?
A very interesting question. The equatorial latitudes are warmer, which one tends to think of as beneficial to humans, and might affect the answer.
I do think Germ theory needs serious modification
More research needed – but it won’t be done because it fits and gave rise to bigpharma. The body is invaded by a pathogen therefore kill the pathogen, thus was bigpharma born.
Wouldn’t it be hilarious if the reality was that viurus in themselves do not cause any illnesses.
Before that thought is mocked read the substacks of “Unbekoming” –
https://unbekoming.substack.com/p/what-is-mumps
New viruses and viral evolution are not driving these infections but changing host susceptibility may be…
…Fits with the conclusions of the Pittsburgh common cold studies carried out several decades ago – “psychological stress is associated with increased risk for developing respiratory illness for persons intentionally exposed to a common cold virus.”
Points an iatrogenic finger at the pandemic, panic, pandemonium of 2020.
It’s an interesting article. It seems to me that the susceptibility theory makes a lot of sense. Having read your ‘Spiked’ book, one of the factors that wasn’t there was how variable our immune systems are round the year, in particular the variation in Vitamin D levels. There has been a lot of published bumf about that (not by the usual government suspects). I suggest the likes of John Campbell and Ivor Cummins have something to say about that.
Although there is not much money in Vitamin D, being a natural automatic product in ourselves when the conditions are right (adequate exposure to ultra violet-B), the fact that we do such a thing (along with other mammals) suggests that it is fundamental – it is not a luxury. Whilst it was originally discovered in the context of the cause of rickets, it probably does a lot more, in a kind of efficient fashion. We are not stupid at that level (even if we are upstairs).
Thanks John. Vitamin D did get a mention in my first book Expired. I think it is only part of the seasonality of our immune response. I don’t emphasise it on its own as our peak vitamin D levels are in September and respiratory viruses are rising substantially by then.

https://www.sciencedirect.com/science/article/pii/S0002916523279964?via%3Dihub#f1
could viral latency be playing a part here, e.g we are pre-infected, and the virus is just waiting for our immune system to dip?
An interesting article, of which the underlying hypothesis is convincing. The last paragraph in particular is great! But throughout it is assumed that viruses, as described by established virology, exist and behave as expounded in that virology, For example, under ‘Evidence for viral contagion’, there is in fact no evidence. The paragraph: “Viral genetic material….” appears to be based on determination by computer modelling fed with very limited partial sequencing of ‘viral’ fragments. And for those who cry ‘Whole genome sequencing’; while the engineering in nanopore sequencing is awesome, the published maximum error rate is about 15% – so, in an RNA virus genome of say 30,000 bases up to 4,500 may be WRONG! The next paragraph says it all; one might add that electron microscopy cannot be used to view living matter, but no matter – viruses are not living matter, even by the accounts of virologists. “At high doses, transmission works…” I was looking forward to reading the method section of the referenced report, but was unable to access the full document. From the abstract it is clear that the study in no way demonstrates contagion. It appears that viral presence was not detected, rather it was inferred from the presence of antibodies. … Read more »
An excellent read.
Viruses are in our bodies all the time. Don’t give them an easy ride – eat meat, green things, lemons, make sure you’re hydrated, exercise, and above all – enjoy your life, don’t stress too much and ….
Spend less than you earn
Avoid debt
Invest the rest
Wasn’t there a study done which revealed that the vast majority of Scandinavians have the HIV virus in their bodies and never knew about it, and have never suffered any illness from it?
Another excellent article!
To date, virology has not followed Koch’s or Rivers’ postulates to determine viral contagion. Until this has been done, the theory of pathogenic viruses remains unproven.
Because of the above, no tests (e.g PCR/antigen etc) exist that have the ability to determine causation of disease symptoms.
Labelling those who question the existence of pathogenic viruses ‘deniers’ is disingenuous, and stiffles discussion and debate. Similar to virology’s circumvention of the scientific method, we must not circumvent logic.
If scientists and medical doctors were honest, they’d observe that viruses (and other cellular debris) are a result of detoxification, not pathogenic.
Observations of a man on an omnibus: ‘Human behavioural changes like school terms made no difference to peaks in lockdown.’ But the Amnesty report ‘As If Expendable’ 2020 points out: ‘25,000 patients, including those infected or possibly infected with COVID-19 who had not been tested….discharged from hospital into care homes between 17 March and 15 April’ which resulted in ‘2 March (to)… 12 June 2020, 18,562 residents of care homes in England died with COVID-19, including 18,168 people aged 65 and over….almost 40% of all deaths involving COVID-19 in England during this period.’ The threat from covid was to the elderly and infirm, 99.95% recovery rate for those under seventy. General human experience indicates that Influenza Like Illnesses spread via human contact coinciding with the start of school/university terms, families travelling/gathering for religious festivals etc. which does seem to pretty much explain the regularity of epidemic peaks ‘Every early January…Often early April…Sometimes in July…Every late October’ I certainly heard reports of severe colds and respiratory infections October 2019 coinciding with the return of Chinese students to a nearby university. We also probably know: ‘manual transmission in a group playing poker was prevented by using splints or large plastic collars; yet… Read more »
‘Compared to Sars and Mers we are talking about a coronavirus that has a mortality rate of 8 to 10 times less deadly to Sars to Mers. So a correct comparison is not Sars or Mers but a severe cold. Basically this is a severe form of the cold.’ ‘right now you also have influenza going around so what you want is to be able to rule out influenza so you can treat the patients correctly for coronavirus.’ ‘Three things the virus does not like 1) sunlight 2) temperature and 3) humidity.’ ‘Sunlight will cut the virus ability to grow in half so the half-life will be 2.5 minutes and in the dark it’s about 13m to 20m. Sunlight is really good at killing viruses.’ ‘the southern hemisphere will not see any great infections rates because they have lots of sunlight and they are in the middle of summer.’ ‘In regards to temperature, the virus can remain intact at 4 degrees or 10 degrees for a longer period of time. But at 30 degrees then you get inactivation. And High humidity the virus doesn’t like it either. That’s why I think Sars stopped around May and June in 2003 –… Read more »
“General human experience indicates that Influenza Like Illnesses spread via human contact…”
This is not a scientific approach, it’s merely a belief based on a very convincing observation. When the scientific method is appropriately applied to covid-19, SARS-CoV-2 and associated mortality, one has to conclude there was no respiratory pandemic at all.
People were dying, but not because of a virus.
It is very much not a scientific approach as I pointed out in my very first sentence. Nevertheless, it has been widely empirically observed. ‘We found (from 25 studies) low evidence, that transmission via hands and fomite followed by self-inoculation is the dominant transmission route in real-life indoor settings. We found moderate evidence, that airborne transmission either via large aerosols or small aerosols is the major transmission route of rhinovirus transmission in real-life indoor settings. This suggests that the major transmission route of RVs in many indoor settings is through the air (airborne transmission).’ https://www.sciencedirect.com/science/article/pii/S0196655322008665 ‘In volunteer studies with coxsackievirus A21 it was shown that colds could be transmitted from one end of a long room to the other when only air contact was possible (Couch et al., 1970). We demonstrated how Coxsackie A21 virus, which is very like a rhinovirus, is shed as drops and droplets into the air by a subject with a cold and that similar droplets infect the nose efficiently when inhaled (Buckland et al., 1965). However, there was very little virus in saliva and so little became airborne when talking. In 1973 Hendley and colleagues at the University of Virginia reported that virus could get… Read more »
You, like many others, start your reasoning based on a false premise that there’s a viral pathogen that is passed between humans. This is yet to be established using Koch’s or River’s postulates. As I’ve mentioned before, there has been zero isolation and/or purification of a viral pathogen.
The literature is full of circular reasoning, false inferences and beliefs, propped up by layer upon layer of circular referencing. None of the research/trials you linked to (or free papers they referenced) demonstrated human-to-human transmission. If contagion is a real biological phenomenon, it should be demonstrable under controlled conditions, especially through natural exposure routes. Yet across more than a century of experimentation, this has consistently failed.
I’ll say it again, contagion is a nothing more than a very convincing observation, supported by pseudo-science.
It really is turtles all the way down.
I don’t even know what a ‘viral pathogen’ is.
But I do know that a common cold (coronavirus) is mainly contracted via aerosol transmission and mainly remedied by rest (and then, after two days, gentle exercise in the open air), allowing the immune system to do its work.
I know this from personal experience. I know exactly how I contracted such a ‘common cold’, when and where I contracted it and who I contracted it from…and I know how I recovered from it.
Do I need to know much more than that?
No; I don’t.
Should the government have known that? Yes, certainly they should have.
Did they need to know much more than that?
No.
All the rest of the £500 billion nonsense was the wittering incompetence of an over mighty, self important and, in many cases, venal public sector that requires draconian downsizing and systemic reform.
No doubt you still believe Santa puts the presents under the tree… or was it someone else?
Where is the demonstration of coronavirus isolation and purification?
Belief built on indirect evidence is illogical, irrational and anti-scientific. The concept of a ‘pathogenic virus’ has not been established through direct empirical observation, only through layers of indirect reasoning that does not meet modern scientific standards.
Virology as a ‘science’ must not be allowed to circumvent logic.
And I certainly do not know who ‘Santa’ is either.
I really don’t give a flying fig whether a coronavirus has been isolated and purified. Nor does I give a flying fig for the idea of ‘pathogenic viruses’ whatever those may or may not be.
I do care that the common cold could kill me.
That is why I have read ‘The View From the Common Cold Unit” and so much else and am happy to contract the common cold on a regular basis to update my immune system. I have no idea how that works (nor do I need to). It is enough that it does work.
Nor do I or most people give a flying fig for ‘virology’, whatever that may or may not be.
The general public want a health service that is true to its first principles, nothing more; one that concentrates on practical measures to improve the health of the nation.
They would be much better served by a universal social insurance based health system as set out by the I.E.A. in its paper, ‘Universal Healthcare Without the NHS’.
I’ve tried my best to communicate with you, but some people just don’t (or can’t) understand.
I wish you the best in health. Have a good day.
You have tried to patronise.
You have been rude.
Some people look into the mirror but see nothing, some do not believe what they see so delude themselves, others will not look at all.
The lucky few just know what is good for them and are content with that.
I would be interested to know whether blood type is a factor in the spread. I’m a complete amateur of course but I did read somewhere that O and -O blood type gives some immunity due to the lack of A and B antigens.
Your question is based on a false premise that some ‘thing’ (a pathogenic virus) spreads between humans.
Could extracellular vesicle production be part of the answer. Why colds and flu viruses are more common in winter | CNN https://share.google/kCZ48oS564eD0QZ6a
It is such an intriguing conundrum.
So many unanswered questions.
Interesting article from Dr Craig. Importantly, she presents strong evidence for contagion. Critics of the prevailing germ theory, including advocates for various types of terrain theory, are weakest at this point. Environment factors, both internal and external to the body, are very important, but direct contagion from another human individual appears to be irrefutable in some cases. Perhaps the key to the mystery is research carried out by Russian scientist A G Gurvitsch, beginning in 1923. Briefly, Gurvitsch et al demonstrated that living organisms affect one another – the rate of cell division for instance – even when completely separated by quartz glass, so that physical micro corpuscles – e.g. bacteria or viruses – could not migrate from one to the other. However, the effect ceased when using ultra-violet (UV)-opaque glass, leading to the conclusion that electromagnetic radiation in the UV range was responsible. Gurvitsch et al further concluded that this was mitogenic radiation, i.e. bio-photons. Gurvitsch also used chemical, thermal, mechanical or electrical treatments to stress inducer cells, terming the radiation emanating from stressed cells “degradation radiation”. Experiments on stressed cells – analogous to illness or disease – were continued by other researchers, notably the Russian research group of Kaznacheev (1960s-80s) which investigated how different stressors… Read more »
Thank you for that. It is news to me.
It seems that scientist have struggled to replicate the experiment but there are experiments that indicate communication between cells at a distance via exosomes, chemicals.
The light emission point intrigued me and reminded me of the flash of light at conception from zinc.
Light from new life = 450-600nm
Light from cell death = 260-600nm – as if life’s final act includes a higher-energy harmonic and octave up
“… but direct contagion from another human individual appears to be irrefutable in some cases.”
As I’ve already mentioned on this thread, contagion between humans is yet to be proven. Viral pathogens have yet to be isolated and purified, then unequivocally proven to cause disease.
Virology is based on a flawed premise, maintained using circular reasoning and a circumvention of logic i.e the scientific method.
Contagion is a whopping lie that modern medicine is struggling to admit, and society is struggling to accept.
“If we want to predict and prevent illness, we need to stop staring only at the virus and start listening to the human immune clock and the environment it inhabits”.
Rather a grand ambition to predict and prevent illness. What about concentrating on good effective cheap treatments such as Vt. C, D, iodine and clean water and nutrition and leave the human body to balance itself?
Very interesting about the submariners.
These cycles of respiratory viruses have occurred for centuries in the same patterns. How can they have been do consistent if the blame is laid on what we do?
I am only a man on a bus but these cycles do seem, in the main, to coincide with seasonal climatic variations, as Prof. Nicholls points out, above?
Because these viruses are affected by sunlight (UV), humidity and temperature?
‘Conclusion: Young children, rather than meteorological factors, served as the primary determinant of viral transmission. The proximity of 3 large viral waves to school reopening after the summer break suggested school transmission is an important contributor. The significant association of meteorological factors with viral transmission increased the risk further, reflecting the period of the year of maximum transmission. This was seen with as viruses with a clear seasonality but not with viruses with atypical or absent seasonality.’
https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2025.1568049/full
Yet we shut the schools and nothing changed…
Thank you very much for this most interesting article and all your work, interviews, common sense, during the novel common cold coronavirus panic.
You know a great deal more about this subject than I do.
Schools, of course, remained open for key workers children, 14% of total pupils. University students remained at universities. Also the schools were shut 20 March 2020 but SARS CoV 2 may very well have been circulating since Chinese students returned to British universities in October 2019 and certainly from January 2020. Patients with serious respiratory conditions were certainly present in Leeds Oct 2019, having close relatives involved in student lettings. There are over 5,000 Chinese students studying in Leeds.
The Amnesty report, As If Expendable, regarding 2020 NHS hospital clearances, does, at least to the uninformed me, support a significant role for the sudden movement of relatively large numbers of people in causing increased ILI infection rates.
Equally, the Common Cold Unit alluded to the importance of the immune system regarding coronaviruses so would, I’m sure, if it still existed (why not?), very much agree with your final sentence above.
Very many thanks. Most grateful.
Yes – that is something a lot of people have looked at. They are indeed affected by those things but not enough to fully explain what we see.
I certainly would not and could not argue with that.
There really does seem to be a great deal that the human race does not know…alarming, given the confident assertions of Chief Medical Officers, Professors of mathematical biology and others:
‘We are about six weeks into this outbreak and this virus can now clearly spread between humans…It is not SARS. The virus is in a similar family as SARS but this looks different … and the difference is probably it is easier to pass between human beings.’
Jeremy Farrar 23 Jan 2020
And so on and so forth…
You’re right.
Predict is doable – it has been the same for hundreds of years after all!
Prevent is probably not so easy.
Another amazing article from Clair, thank you for all this work and explaining so clearly.
Riddle me this.
If measles is caused by a virus, why in England did mortality decline from its peak level an astonishing 99.96% by the time the vaccine was introduced in 1968?
Ender’s use of tissue culture is NOT proof of viral ‘isolation’, and virologists’ behaviour in claiming such is convenient and practical, but with regard to the claims that are made and the subsequent actions that are carried out against humanity, this behaviour should be viewed as dishonest, improper and immoral.
It seems virology not only circumvents logic, it also abuses the English language.
Here you go: https://dearchurchleaders.substack.com/p/the-story-is-always-half-the-kids
So you also agree a pathogenic measles virus is a myth?
It is nothing like what the Victorians described as “measles” – no.
But there is an associated low mortality rate to this day depending on the nutritional state of the child. Having said that, the places where the measles mortality rate is concerning currently also are places where mercury is still used in traditional therapies.
Did the Victorians accurately describe ‘measles’ and its causes? Did virologist John Franklin Enders ‘isolate” and’ prove’ the existence of a measles ‘virus’ in his 1954 paper “Propagation in Tissue Cultures of Cytopathogenic Agents from Patients with Measles”.
Tissue cultures do not prove existence or causation.
This is definitely a good discussion. I think the question on the existence of ‘pathogenic viruses’ MUST be clarified and robustly proven. This points is upstream of the whole discussion of contagion. If the theory of pathogenic viruses is not proven based on the scientific method then we are really in the realm of beliefs; frankly not very scientific. I’m not a scientist; read the Viral Mania and watched the End of Virology and lots of question marks popped up. No point in calling people names ie deniers and the like. The supporters of the theory should provide unequivocally robust evidence to support it. Then we – including the ‘deniers’ – can have a proper debate. Otherwise the question marks remain.
I am a scientist, and you are 100% correct.
I am from the government and I am here to help.
Dear Dr Craig, I have already bought for family members copies of your book Spiked:a shot in the dark, as I know it is the only book which exposes scientifically the Covid scam. As such, the elite will ensure that sooner or later the book will disappear from libraries. For my own collection, however, and with DS permission, could you kindly advise me where I can purchase a signed copy of the book as all my searches have failed.
Is it mostly the same sub-group that gets influenza? Is there a sub-group that nearly never gets it? Just an innocent question.
Yes. The sub-group that nearly never gets it, we ‘scientists’ call ‘parliament’. The sub-group that never gets it, we call ‘Whitehall’