All the Flaws in the Lancet Paper That Claims to Show Covid is a Greater Myocarditis Risk to Children Than Vaccination
A new Lancet Child and Adolescent Health paper has drawn headlines suggesting that COVID-19 poses a greater myocarditis risk to children than vaccination. A closer look at the data, however, raises serious questions about how those conclusions were reached.
The headlines were that Covid was a greater risk for myocarditis in children than the vaccines. There is solid evidence and from multiple sources that this is not true, so how did this reversal happen?
Before we begin there are three key points that mean this kind of analysis based on diagnostic codes in the medical records – even if done honestly – is not a good measure.
First of all, one study from Thailand found 3% of teenage boys after their Covid boosters had evidence of dead heart cells, measured with raised troponin levels in the blood, while a third had cardiac symptoms. These subclinical signals will not always be picked up in medical records.
Second, it is wrong to focus on only one adverse event to the exclusion of others.
And third, the vaccines did not prevent infection so it is not an either-or sum. Vaccinated children were exposed to more risk, regardless of the risk from Covid.
These are the key issues with the two new studies at a glance:
- Selective framing: The studies presented infection as the greater danger, but avoided comparing post-infection risks in vaccinated versus unvaccinated children.
- Data manipulation: Heavy statistical adjustments and merged age groups diluted vaccine-associated risk.
- Incomplete datasets: The analyses excluded data beyond 2022, despite evidence of ongoing myocarditis cases.
- Uneven comparisons: Timeframes for infection and vaccination were not aligned, biasing outcomes in favour of vaccines.
- Lack of transparency: No raw counts or control checks were shown to validate the models.
- Focus on younger group: The studies did not include Moderna doses nor the people in their 20s who were at highest risk, and made no comment on the greater risk after doses two and three, only presenting data for six months after the first dose.
What was the risk?
Two large national studies, one Oxford-led (Nature Communications, 2024) and one UKHSA (Imperial-led; Lancet Child & Adolescent Health, 2025), analysed data from the NHS in England and both made heavy adjustments. The first showed a myocarditis risk of four per million post-infection in unvaccinated children whereas the later study, which included the second half of 2022, showed a risk of 22 per million post-infection across all children. Why would the risk after infection have risen not fallen when children were vaccinated?
In Nature Communications, the raw data implied roughly 18 myocarditis admissions per million vaccinated adolescents within six weeks of a dose (36-plus cases among around two million vaccinated 12-17 year-olds – the raw data are hidden in the appendix). If you included those not admitted to hospital it would be higher. If you included those who were not diagnosed it would be higher still. However, after regression adjustment, the authors reported only three to five additional cases per million, a downward revision of about three-quarters.
The Lancet analysis, which included the second half of 2022 and was based on a larger dataset, had 250 cases post-vaccine, working out at 19.3 per million for all aged 5-17 years. It too modelled the risk but over six months follow-up, and it ended up reporting 8.5 per million following vaccination, still higher than Nature’s adjusted figure but diluted by combining age groups.
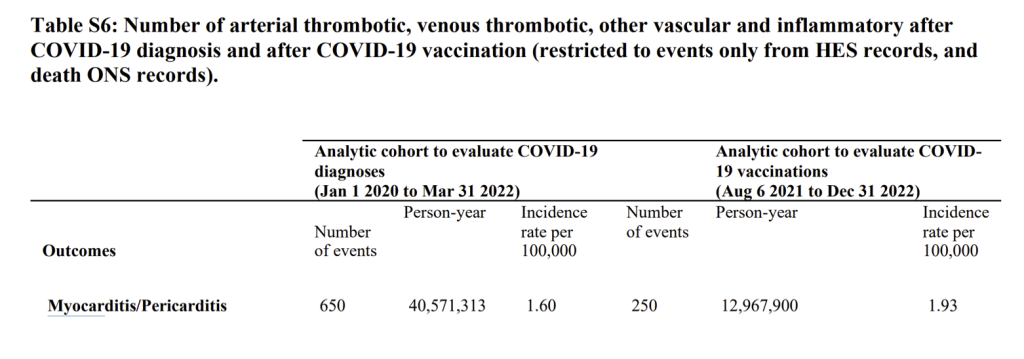
The Lancet group adjusted its 1.60 per 100,000 figure for incidence of myocarditis/pericarditis after infection (16 per million) and presented a figure of 22 per million after an infection. This included the period in 2020 when tested children were disproportionately hospitalised for other conditions. It is striking that the vaccine risk and infection risk are so similar.
Were events double counted?
There is a big problem with the data in that table. There were only 371 myocarditis and pericarditis diagnoses in England between March 2020 and April 2023 in under-18 year-olds. Where did the 650 events these authors are claiming come from? They simply do not exist in the real world.
Table 2 in the main paper included diagnoses outside of hospital (see figure 2). The apparent total number of cases is twice as high in the post infection group compared to table S6 above. Meanwhile, the post-vaccine total is 3.6 times as high. Notably the population-years figure used as a denominator in the post infection group has fallen by a quarter too.
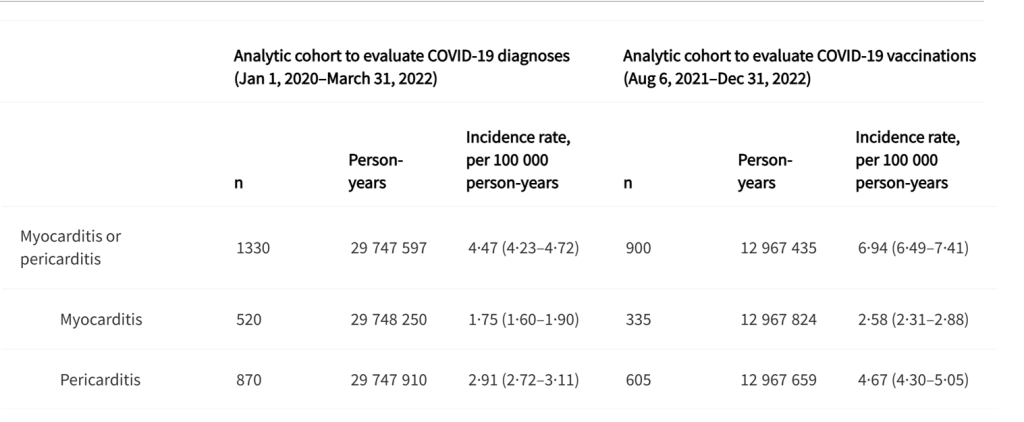
The authors combined data from multiple sources but were not able to deduplicate overlapping records across datasets. Table S6 uses only hospital admissions and death records, whereas Table 2 adds data from A&E attendances. Because events recorded in A&E may also appear in hospital records for the same episode, the inclusion of A&E data could lead to some double-counting of clinical events. Because Table 2 includes events recorded across multiple healthcare settings without episode-level deduplication, the larger numbers may reflect the total number of healthcare encounters related to an outcome rather than the number of unique clinical events. In this sense, the figures can be interpreted as a measure of healthcare encounters per person, rather than unique incident cases. That would imply the post-vaccine cases were seen more often than the post-infection ones.
Ultimately, the raw data in this table look even worse than in table S6. It was the adjustments that got them the headline.
Now, any decent analysis would have presented risk after infection separately for the vaccinated and unvaccinated. You can bet they would have done that if it had looked favourable for the vaccine. They did not. They never do.
Importantly, the risk of infection is low in any given year but 100% of the risk from vaccination is included with every vaccine. They did present some comparison between vaccinated and unvaccinated. Here are the totals for conditions from 2020-2022 in each group. Clearly the unvaccinated have had more time to acquire diagnoses. The overall risk in the vaccinated of myocarditis was four times as high and the risk from pericarditis was three times as high.
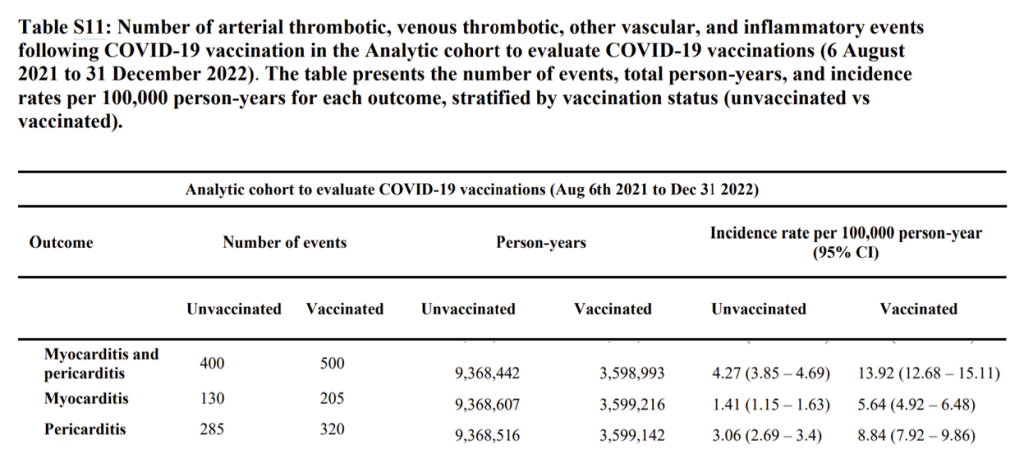
Because vaccination coverage rose from nearly zero to about 30% during the study period, vaccinated person-time should represent only about 20% of total exposure. In Table S11 the vaccinated represent 27%. Based on the event data (e.g. total PIMS-TS count) Table S11 appears to cover only August 6th 2021 to December 31st 2022. The result of a higher denominator would be to suppress rates in the vaccinated group.
When data are heavily adjusted like this, contradictions appear. There were many reasons to question the accuracy of the analysis, e.g. why were females and males said to be at equal risk when no other study showed that for this age group?
Were data over-adjusted?
The paper showed that children aged 5 to 11 years-old had double the risk of myocarditis/pericarditis (adjusted hazard ratio 11.27 in week 1) compared to the teenagers in this analysis (adjusted hazard ratio 5.48). This was not mentioned by the authors anywhere in their paper but simply reported in a table in the appendix. The NHS data do not show a rise in myocarditis in the primary school age group but do in teenagers (and in older people, and it is continuing). The result is likely spurious from overadjustments.
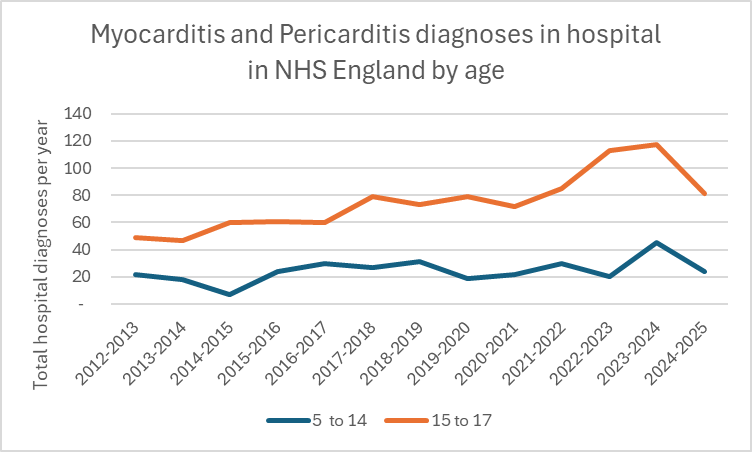
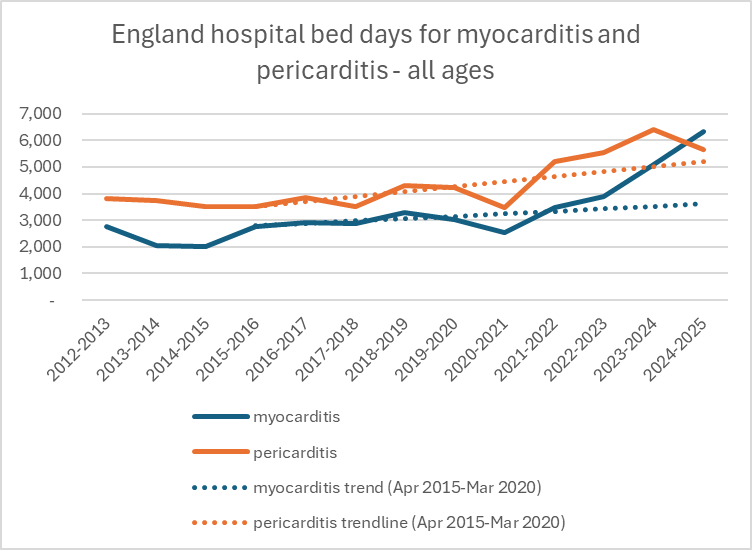
It is clear from national data that myo- and peri-carditis cases did not increase in 2020-2021, only rising steeply after April 2021 i.e., as the younger cohorts were being vaccinated.
What they did not do
- They did not include Moderna doses nor the people in their 20s who were at highest risk.
- There was no breakdown of post-infection risk by vaccination status.
- There was no inclusion of data beyond 2022, even though NHS figures show myocarditis continuing to rise.
- There was no separation by dose number, despite known dose-response effects.
- There were no raw rates; instead of the standard ‘unadjusted vs adjusted’, the paper offered only “minimally” and “maximally” adjusted models.
- There was no control condition to verify that the adjustments behaved reasonably.
Each omission leans in the same direction: infection appears more dangerous, vaccination appears more benign.
There was a string of biases
A Biased sampling of ‘sick’ children
- They minimised conditions after vaccination by excluding the majority of sick vaccinated children who were injected before August 6th 2021 while including sick children in the unvaccinated comparison.
- They inflated conditions among those with a diagnosis by including all ‘cases’ from spring 2020 when only children testing positive were those with access to tests because they were already patients. That is why conditions were present on day zero after diagnosis.
- They combined control groups and compared rates after diagnosis to the same people before diagnosis as well as to the undiagnosed, but failed to show the analysis for each control group
- Similarly the vaccinated were compared both to the vaccinated prior to vaccination and to the unvaccinated, but the analysis combined the two.
B Age groups
They used age 0-18 for diagnoses but 5-18 for vaccination comparison.
C Time frame
- Infection follow-up ran January 2020 to March 2022
- Vaccination follow-up ran August 2021 to December 2022
These are not like-for-like. There is no good reason to do this, especially when no attempt was made to present unvaccinated infection risk.
To minimise the risk from vaccines they diluted the impact over a six month window and looked at risk after first dose rather than the highest risk in period immediately after dose 2 and 3.
The risk was not from infection alone. There was something else that was happening after infection.
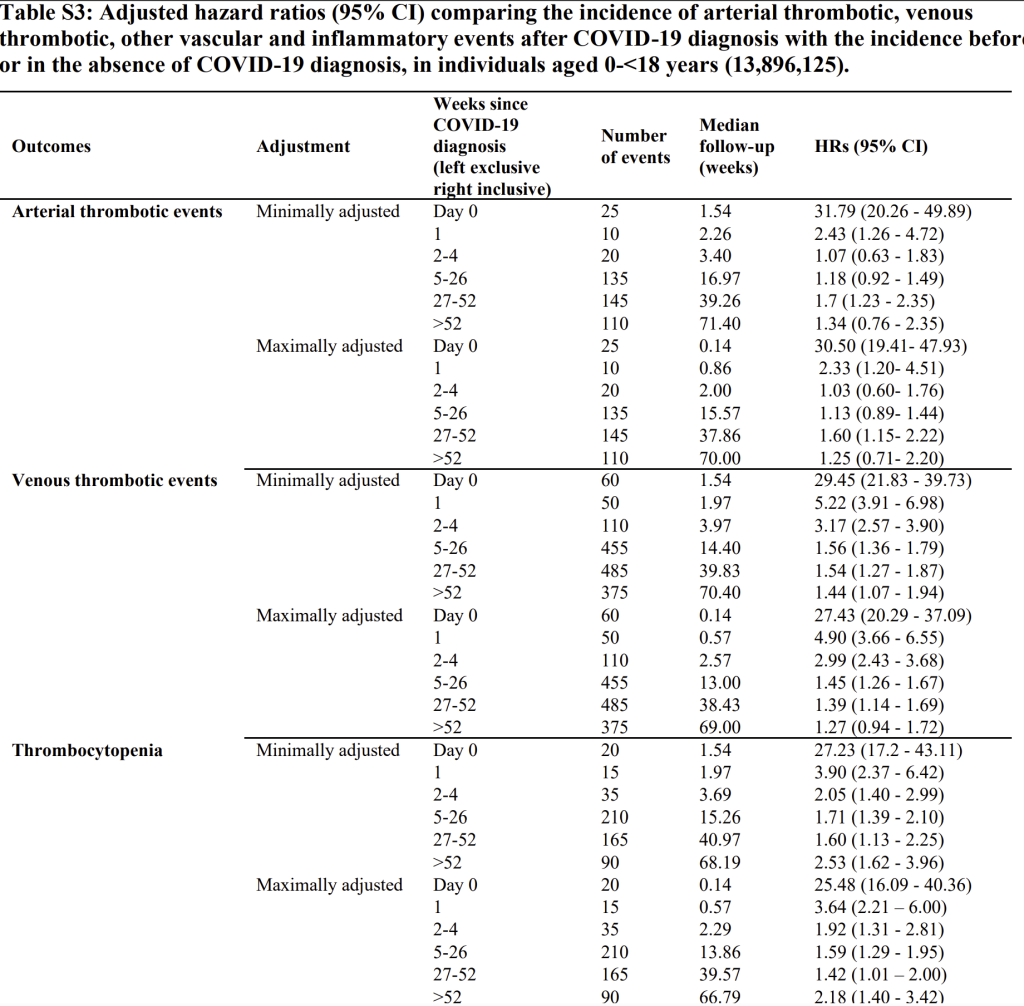
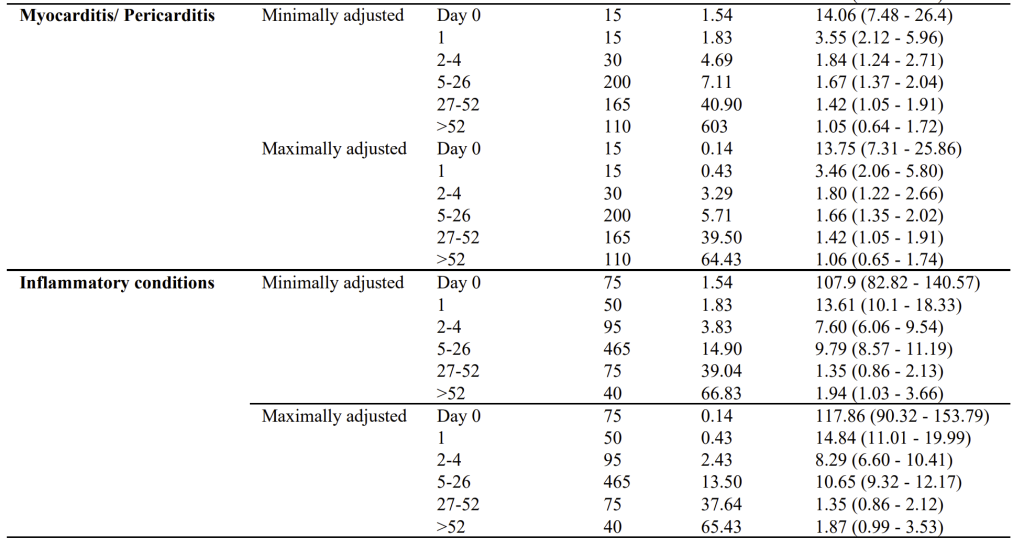
In Table S3 the authors present the risk in different time periods after infection. The first thing to note is the high number of events at day zero. This suggests a disproportionate number of children had the adverse event before testing positive i.e., they tested positive when admitted for one of these conditions. After day zero, rates declined sharply but remained statistically above the over-52-week baseline for several outcomes during the early post-exposure weeks (e.g. weeks 5-26). It is impossible to determine from these data whether this represents a continuing decline from the day zero artefact or a true association with the exposure.
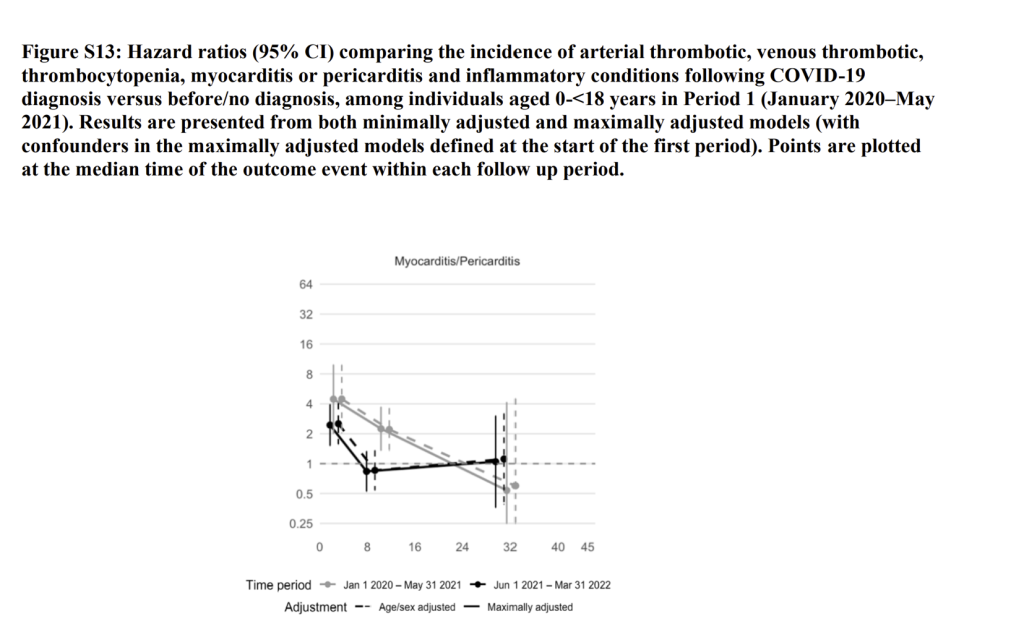
How could the risks arising from an infection appear so late on?
The risk is clearly only early on from their own graphs. Here you can see the hazard ratio plotted against ‘week since diagnosis’, comparing those who tested positive with both the same individuals pre-diagnosis and the undiagnosed. The grey line includes the period where test-positive children were disproportionately hospitalised for other conditions and has a very high day zero rate. The black line is for the later period from June 2021. The claim of a sustained risk long-term from infection is not supported by this graph.
D Flaws in the Nature paper too
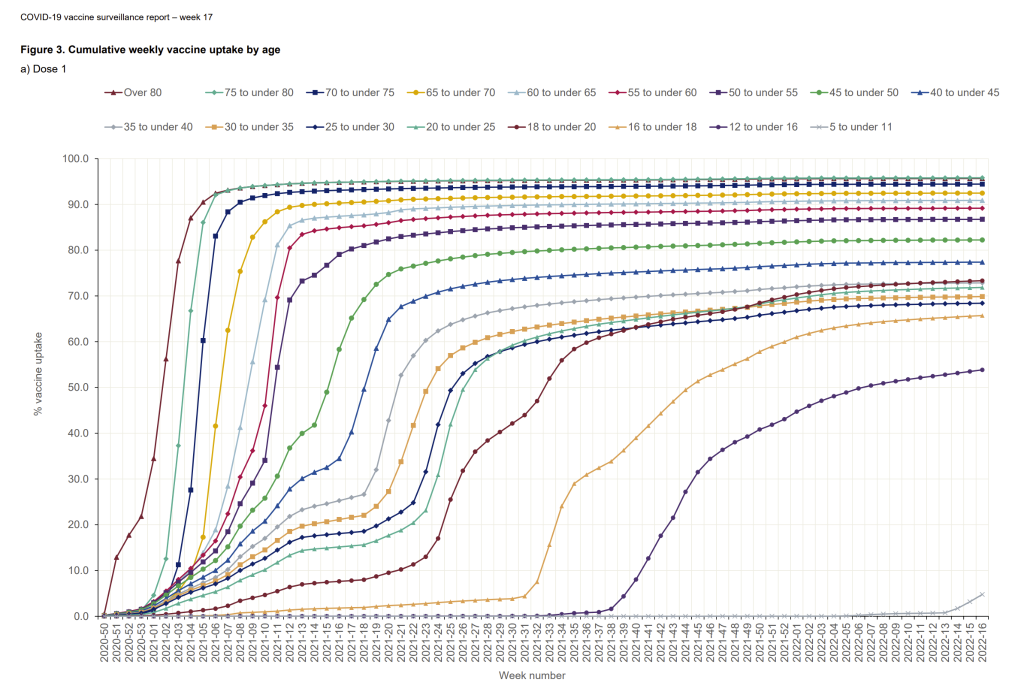
The Nature paper we are using as a ‘control’ was not flawless, e.g. it claimed that 86% of 12-17 year-olds received a first dose, which does not tally with UKHSA data (see below). Higher denominators reduce the rates claimed regarding risk.
This same Oxford group had previously published a paper looking specifically at myo- and pericarditis, which has been widely misquoted as stating that risk is higher after infection than vaccination. But in its own abstract it showed that in “men younger than 40 years old, the number of excess myocarditis events per million people was higher after a second dose of mRNA-1273 than after a positive SARS-CoV-2 test (97 [95% CI, 91–99] versus 16 [95% CI, 12–18])”. This is a six-fold difference. When the authors were contacted for a breakdown by age bands in the younger cohort, they stated numbers were too small! A six-fold difference is not one to be ignored and it may have hidden a higher ratio in younger age groups. This was the Moderna rather than the Pfizer BioNTech product, but of course it is Moderna which is now in receipt of massive government funding for its new mRNA research and production facility near Oxford.
Conclusion
The latest analyses from Oxford and UKHSA/Imperial were presented as reassuring evidence that vaccination reduced myocarditis risk compared with COVID-19 itself. But the methodological choices, uneven time frames, merged age groups, missing raw data and selective comparisons all led in one direction: making vaccines appear safer than they were. The overlooked patterns in the data, including several years of higher risk after vaccination, reveal a more troubling reality. Science should be transparent, even when the findings are uncomfortable. The real story is not about a virus versus a vaccine, it is about the importance of honest analysis and the consequences when data are adjusted to fit a preferred narrative. Until we confront that, we will keep repeating the same mistakes and get the same misleading headlines.
Dr Clare Craig is a diagnostic pathologist and Co-Chair of the HART group. She is the author of Expired – Covid the untold story. This article was first published by HART.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
The more people who see this article the better.
I saw this a couple of days ago from HART and added it as number 99 to my list of studies, articles and scientific papers (many peer reviewed) that have been written or scrutinised by highly qualified medical and scientific professionals and show the harms of the Covid experimental jab.
https://classicrecords1.wixsite.com/the-sceptic/post/covid-vaccine-harms-list-of-studies-and-scientific-papers-and-articles
You are correct. I have done the same. The problem is that, if it was sent to ANYONE in the health or medical establishment, NHS, MHRA, MoH etc (e.g. Chris Witless or Streeting), it would simply be binned without reading. They would not permit themselves to challenge the narrative, exercise critical thinking or even consider the possibility that the death jabs are not ‘Safe ‘n’ Effective’. All those responsible for the criminal behaviour of the Government and Medical Authorities / Regulators will have to be either dead or long-retired before the truth is widely admitted and accepted; c.f. the many other medical scandals of the past (e.g. contaminated blood).
It’s not just the medical establishment that ignore the evidence of the Covid jab harms.
I’ve made the list available on most of the main stream media facebook pages when they post a Covid related article and the vast majority of the general public scoff at the idea of widespread harms.
I think they are in denial that they may have a ticking timebomb inside them that was self-inflicted albeit at the advice of the government and medical and scientific so-called professionals.
As ever, the devil is in the detail – and in the cognitive bias of the truth twisters of Imperialist College, South Midland Poly and UK Health Insecurity
Where’s peer review when you need it?
More to the point, what connections do the researchers have to the pharmaceutical industry.
Yes bought by Pharma, as was Pharmament (used to be called parle-ment),
Viruses don’t exist. Send an FOI to the HSA and ask for proof of isolated, purified, real genomes. Zero exist.
Even if they did exist ‘viruses’ are dead RNA and can’t cause anything – including a heart attack.
But the quackcines did and do. Children magically contracted heart issues right after the stabs. Funny that.
No one had ever heard of mycarditiis before the poisons were rolled out.
Yep, myocarditis, pericarditis, Guillain Barre syndrome and the list of 300 side effects from the covax that I wish I had kept were all new ones on me.
‘The real story is not about a virus versus a vaccine…’
The common cold, Influenza Like Illnesses (ILI) generally (and covid is a common cold coronavirus), can cause myocarditis.
‘Potentially cardiogenic SARS-CoV-2, adenovirus, enterovirus, or influenza virus infections are reasons for a break in training…’
https://pmc.ncbi.nlm.nih.gov/articles/PMC11282332/
So once covid is acknowledged, as it should be, as another common cold corona virus: ‘an athlete with a common cold could train and compete but the decision is based on a personalized process between the athlete and the medical team which should also contain expertise in infectious diseases.’
Then the matter becomes straightforward: are covid vaccines safe?
To my personal knowledge, they are not……..
This is a classic example of one of the major benefits of the COVID crisis – that it has resulted in the deconstruction of published scientific research that was inadequate (the research, that is, not the deconstruction). This is because science is now exposed to an enormous cohort of peer reviewers as never before. From COVID to climate change nothing escapes scrutiny of the highest order.
It has certainly educated us with regard to confidence in some professions, and has encouraged scepticism. Could be good, if we manage it effectively.
Thank you Dr Craig for keeping up the fight against those who would harm children rather than admit the truth. God bless you.
Hear, hear. There is a very interesting interview with her on John Campbell’s videos within the last week, in which she and Dr Tim Kelly talk about the serious risks of folic acid which will be compulsorily added to flour some time next year. Another eye opener. My eyebrows will soon be merging into my hairline at this rate.
Is folic acid being added to bread or flour?
A quick search seems to indicate that it will be added to non-wholemeal flour, which sounds promising, if it is true. But wedges have thin ends…..
The Lancet paper is funded by the Wellcome Trust and British Heart foundation which supported the covid vaccines and jabbing children. The Chief Medical Officer also overrode the vaccination committee to authorise their vaccination. It is obvious that they needed a reference that supports their position. As the truth is coming out in the USA, their malfeasance in the UK is being exposed. These are the medics who continued using up stock of the AZ vaccine for months after it was banned in Europe after being found to cause blood clotting and adverse reactions at twice the rate of the mRNA poison.
Can you write a letter to the Editor of the Lancer?