Scientists Are at Last Uncovering the Links Between ME, Long Covid and Long Vaccine
The medical profession has often labelled as psychosomatic problems which it does not yet understand. Multiple Sclerosis was once regarded as a sign of female hysteria before the degradation of the brain’s myelin sheath was discovered. The shaking hand in Parkinson’s was once considered the result of not masturbating enough before a chronically lowered dopamine output was instead identified as the cause. Freud’s theories of psychogenic illness have cast a long and cruel shadow and have arguably been nowhere more damaging than on the most enigmatic condition of all: ME (Myalgic Encephalomyelitis), also known as Chronic Fatigue Syndrome (CFS).
Sufferers complain of debilitating weakness, loss of stamina and a profound worsening of symptoms after physical exertion. This worsening is termed ‘post-exertional malaise’ (PEM) and leaves many patients too ill to leave their beds for days, weeks or even months. The trigger might come from nothing more than walking slightly too quickly up a flight of stairs. The devastating reaction is completely disproportionate to the activity.
And yet routine blood work will often show nothing wrong. While many doctors will wish that they could help these patients, the lack of any obvious abnormality leaves others to conclude that the problem must be ‘all in the patient’s head’. This has sometimes led to well-documented cases of medical abuse and neglect.
But it is highly unlikely that millions of patients around the world, all of whom complain of exercise intolerance and post-exertional malaise, are simultaneously engaging in a hypochondriacal pact. The boundaries of medical knowledge expand in every generation and ME should be best viewed as a puzzle to solve. Dismissing it as psychosomatic is to take the easy way out.
The fact is that ME research has identified many biomedical problems and PubMed lists almost 12,000 papers about the condition. The issue, however, has been that the findings can seem random and disconnected. One study shows a problem in the microcirculation, another in the mitochondria, another in neurological function and yet another in the gut. But if ME is to make any sense as an illness and take its place alongside other chronic diseases, then it cannot be a problem of random occurrences. There needs to be an overall and distinctive pathophysiology.
And that pathophysiology might, at last, have been uncovered.
Over the last few years, two leading ME researchers, Professor Klaus Wirth and Professor Carmen Scheibenbogen, have taken a completely new approach. They started with the premise that there must be a way to connect the seemingly random pre-existing findings in ME research. Why is X happening? And how does it lead to Y and Z? And could Z feed back into X?

Their resulting papers have been a tour de force. They have mapped out a ‘unifying model’ of ME which shows it to be an illness of interlinking vicious cycles. For the first time, ME has potentially been demystified and the dots might – at last – have been joined up.
The resulting pathophysiology is complex and you can read two of their most important papers here and here.
In this article, I will instead consider some of the most striking biomedical problems that can explain the central symptoms of ME: exercise intolerance and post-exertional malaise.
The Core Features of ME
In the simplest terms, ME is an illness of reduced blood flow throughout the body, or global hypoperfusion, and of a highly dysfunctional cellular and mitochondrial state. In the proposed model, these two problems drive each other. The hypoperfusion leads to the cellular deterioration but the latter, once established, only further intensifies the hypoperfusion.
The reduced blood flow is driven by a range of interlocking factors including low blood volume, vascular and cardiac autoantibodies, dysfunctional capillaries and the widespread presence of microclots.
Meanwhile, the cellular dysfunction involves an ion disturbance within the muscle cells. That disturbance causes an excessive accumulation of intracellular sodium and, at times, an overload of calcium. The former problem primarily causes very weak muscles. The latter problem is more serious. Muscle calcium overload can cause cell death, mitochondrial damage and, for Wirth and Scheibenbogen, is likely the primary mechanism behind post-exertional malaise.
From these problems alone, we have a clear basis for an illness of exercise intolerance. How can your muscles work when they do not receive enough blood and oxygen? And if exercise leads to the devastating consequence of muscle calcium overload, how can your muscles recover sufficiently for further activity?
Clear Evidence of a Biomedical Pathophysiology
All that might sound a bit abstract. Let me now show you four clear ways in which some of the aforementioned problems play out in the patient’s body.
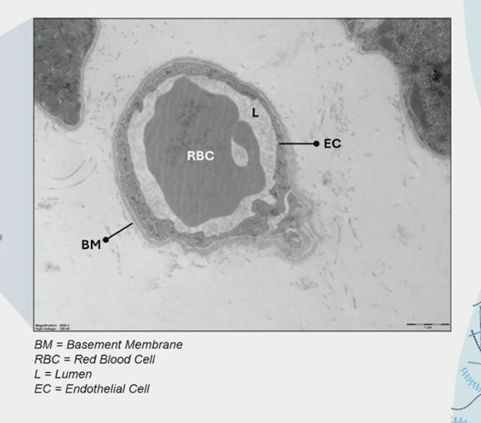
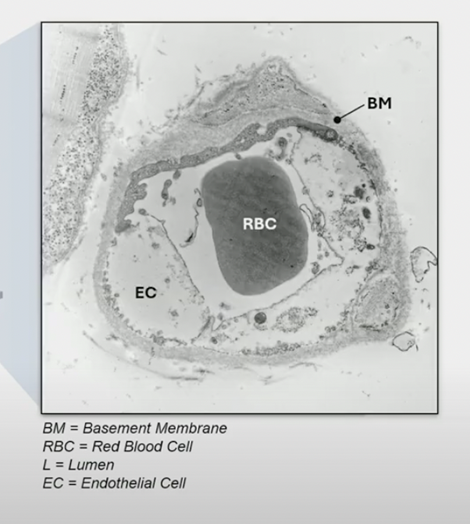
In relation to the hypoperfusion (reduced blood flow), one issue concerns a dysfunction within the capillaries supplying the muscle tissues. In ME, the outer layer of the capillaries – the basement membrane – has become significantly thicker. This creates a kind of barrier that lowers oxygen transfer into the muscles. These changes have been identified under electron microscopy and you don’t need to have a medical degree to spot the difference between a healthy capillary and one with ME:
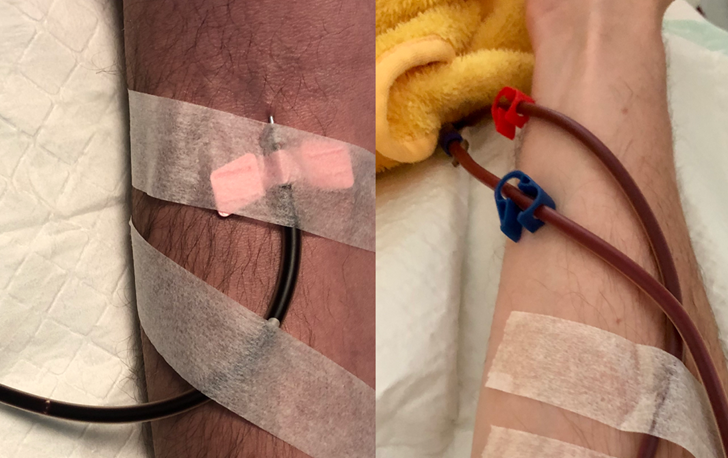
Microclots, meanwhile, represent another key problem. Stemming from the pioneering work of Professor Resia Pretorius, these microscopic clots are too small to cause a stroke but so numerous that they can condense the blood, render it sluggish and provide a further reason for reduced tissue perfusion. Anecdotally, many patients report that their blood looks darker, a likely consequence of its increased viscosity. This was noted in my case too when I travelled to an excellent dialysis centre in Germany for HELP apheresis treatment, a blood-washing procedure that thins the blood using heparin. The change in the colour of my blood after my treatments was striking:
However, the most physiologically devastating component of the hypoperfusion comes from a reduction in total blood volume. One paper showed that housebound ME patients have on average 1.2 litres less blood than a healthy person. If someone were to lose that much blood after a car accident, no doctor would diagnose a psychosomatic problem. But testing blood volume is elaborate and expensive and doctors are rarely taught that ME patients can develop such a problem simply because of their chronic illness.
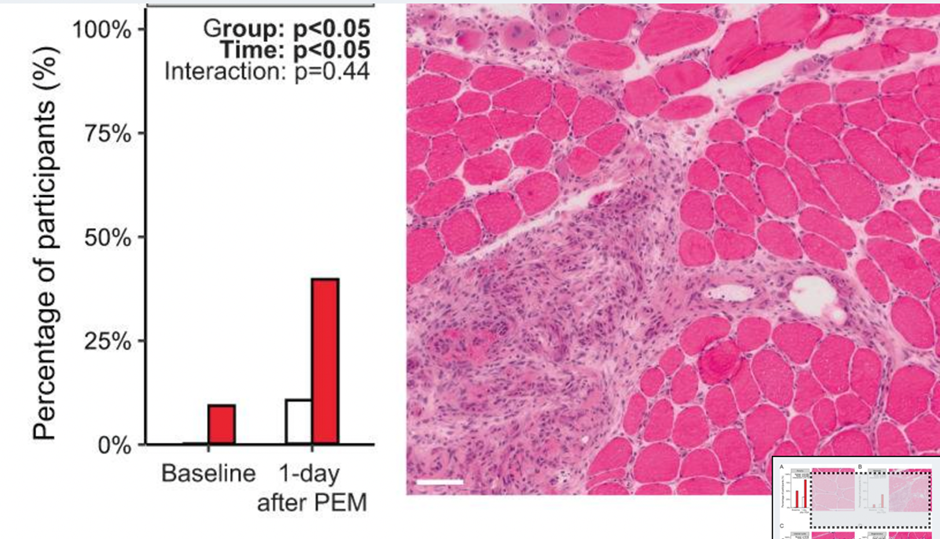
Finally, at a cellular level, a trailblazing team in the Netherlands has found that, during post-exertional malaise, muscle tissue can actually become necrotic (i.e., dead or dying). For Wirth and Scheibenbogen, this finding was crucial as, when the full possible reasons for such exercise-dependent tissue necrosis are analysed, it is only cell death from muscle calcium overload which can provide an explanation. As any disease model must be able to account for such a key finding, this adds great likelihood to the probability that Wirth and Scheibenbogen’s ME hypothesis is correct.
These examples should dispel the oft-cited myth that there is nothing biomedically wrong with ME patients. Rather, the issue has been that standard tests are simply not equipped to capture the illness. Up until now, the situation has been analogous to a doctor examining a patient’s elbow, declaring that all is fine, when all the while the patient has a broken leg and is screaming in agony.
Developing the World’s First ME Medication
There is no officially approved treatment for ME. Patients have instead relied on repurposed medications (such as Low Dose Naltrexone). However, if you – at last – know what the problem is, then you might actually be able to treat it. Wirth and Scheibenbogen’s unifying model – which explains the interrelationship between the aforementioned problems and many others besides – could therefore provide grounds for a truly effective medication for the first time.
Indeed, Professor Wirth has identified a compound, Mitodicure, which aims to interrupt the cellular dysfunction underpinning post-exertional malaise. Of all the pathomechanisms in the illness, Prof Wirth regards post-exertional malaise as the most important to target. PEM heightens and sustains the disease mechanisms and, by preventing it, the body might be able to put its resources more easily into healing. As Wirth has said: “Healing and improvement require the absence of PEM. Our aim is healing the disease and our drug is meant to interrupt the vicious cycle. As soon as the mitochondrial situation has fully recovered, the patient should be healed.”
It is too early to know if Wirth’s concept will succeed but what is clear is that, if we finally have a coherent model of ME, then therapies based on that model could help patients far more effectively than ever before. (For those interested in a more comprehensive explanation of this therapeutic concept, see Wirth’s presentation at the recent Charité Berlin conference.)
A Global Unmet Need: ME, Long Covid and Long Vax
The global figure of ME patients is often put at 17-24 million, although some suggest that this is a significant underestimate. The number of ME cases has certainly risen significantly since the Covid pandemic and many ME researchers regard post-Covid ME to be the most severe form of Long Covid (while allowing for the fact that there exist non-ME forms of the disease, due to pulmonary sequelae for example). Similarly, Long Vax, while often involving specific issues like pericarditis, can ultimately also manifest as an illness of exercise intolerance and post-exertional malaise. While the ultimate end-point pathophysiology of ME is similar between all patients, any significant assault on the body – whether from a virus, vaccine, trauma or other stressor – can trigger the disease.
The politicisation of both Long Covid and Long Vax patients from both sides of the Covid aisle has been frustrating to witness. One side claims that Long Covid is a myth and simply a term to ‘cover up’ vaccine injuries. The other, meanwhile, has cruelly and bizarrely stigmatised Long Vax patients as anti-vax conspiracy theorists.
We should not turn enormous human suffering – whether triggered by a virus or vaccine – into a political football. Apart from anything else, it only perpetuates the decades of neglected research into ME. If governments had prioritised such funding, would so many post-Covid and post-Vax patients be suffering now? The real blame rests with those in power who turned their backs on ME patients over decades.
The ME Narrative Needs to Change
But there yet remains a chance to turn the ship around. ME is discussed more prevalently in the media, such as the tragic death of Maeve Boothby O’Neill and the recent DECODE-ME findings which show a genetic predisposition to the illness. The UK Government’s ME delivery plan is a step in the right direction, while in the USA RFK Jr and Professor Bhattacharya recently sat down to discuss solutions for Long Covid.
However, these things are not enough. Too many patients are currently lying in darkened rooms, some unable to swallow and tube-fed. This situation is not a joke and would not be tolerated for any other disease. ME is not being ‘tired’ and its second – completely ludicrous – name ‘Chronic Fatigue Syndrome’ has utterly failed to convey the seriousness of the disease. To quote American author Laura Hillenbrand: “ME/CFS is to fatigue, what a nuclear bomb is to a match. It’s an absurd mischaracterisation.”
We need to get very clear about our end goals in order to maximise the speed of the necessary change.
The first should be that ME is not a disease of random occurrences but instead has its own distinct and clear pathophysiology.
And the second is that we need to develop treatments based on that pathophysiology. Whether it is Wirth’s Mitodicure or other compounds yet to be developed, it is these treatments – not off-label medications which just target problems ‘around the edges of the disease’ – which could actually make the greatest difference.
ME need no longer be considered an enigmatic disease. Now is the time to increase funding dramatically, test potential therapies and – at last – reduce the suffering of a patient population whose cries for help have gone unheard for far too long.
Patrick Ussher is from Ireland and has had ME for over seven years. He is author of the book Understanding ME/CFS and Strategies for Healing which explains the unifying model of Wirth and Scheibenbogen in an accessible way. He also has a YouTube channel about ME/CFS research and treatments (including an interview with Professor Wirth), and his work has been featured in the Irish Times, the Medical Independent and the Conservative Woman. He is also author of books on Stoicism and Buddhism and is a composer of contemporary classical music. For more about Patrick, see his personal website.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
If you want funding, perhaps best to avoid saying that there is such a thing as “long vax” (safe and effective).
Oh golly gosh. The saintly medical profession have failed us. Again
I wish it were funny. Instead, bad decision making by your top gov’ts medical advisors, it is bankrupting your country. Did any of the apologise for their poor advice? No I did not think so. Instead they were catapulted to top jobs with big pharma.
How on earth did your gov’ts top medical advisors allow the millions of mRNA Covid vaxxes to be administered, when they had absolutely no idea whether they were safe or effective? Something so simple, ignored. Now GPs get to deal with post vaxx injuries in the millions, and not a word of apology from your gov’t or from their “top” paid medical advisors. One big mess. Never again.
The only way for never again to be the case is if we all refuse to take any drug or treatment that hasn’t been explained to us and that we have given fully informed consent.
I think the various health services would slow down massively and probably many medical staff would self-combust.
I wonder if in all the work done on ME anyone has looked at organophosphates? These were developed as bioweapons and nerve gases but are in regular use as pesticide treatments for both plants and animals. I have known people who suffer from ME getting relief by sticking to an organic diet. You may – or indeed these days may not – be surprised to learn that while all the pesticides used on our food are at the recommended safe dose, nobody has looked at what happens when these safe doses are mixed up in our diets.
Organophosphate Poisoning – symptoms and treatment – DoctorMyhill
Great article.