CDC Quietly Admits to Covid Policy Failures
In so many words — and data — CDC has quietly admitted that all of the indignities of the COVID-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, and especially the vaccines; all of it failed to control the pandemic.
It’s not like we didn’t know that all this was going to fail, because we said so as events unfolded early on in 2020, that the public health management of this respiratory virus was almost completely opposite to principles that had been well established through the influenza period in 2006. The spread of a new virus with replication factor R0 of about 3, with more than one million cases across the country by April 2020, with no potentially virus-sterilising vaccine in sight for at least several months, almost certainly made this infection eventually endemic and universal.
COVID-19 starts as an annoying, intense, uncomfortable flu-like illness, and for most people, ends uneventfully two to three weeks later. Thus, management of the COVID-19 pandemic should not have relied upon counts of cases or infections, but on numbers of deaths, numbers of people hospitalised or with serious long-term outcomes of the infection, and of serious health, economic and psychological damages caused by the actions and policies made in response to the pandemic, in that order of decreasing priorities.
Even though numbers of Covid cases correlate with these severe manifestations, that is not a justification for case numbers to be used as the actionable measure, because COVID-19 infection mortality is estimated to range below 0.1% in the mean across all ages, and post-infection immunity provides a public good in protecting people from severe reinfection outcomes for the great majority who do not get serious ‘Long Covid’ on first infection.
Nevertheless, once the COVID-19 vaccines were rolled out, with a new large wave of the Delta strain spreading across the U.S. in July-August 2021 even after eight months of the vaccines taken by half of Americans, instead of admitting policy error that the Covid vaccines do not much control virus spread, our public health administration doubled down, attempting then to compel vaccination on as many more people as could be threatened by mandates. That didn’t work out too well as seen when the large Omicron wave hit the country during December 2021-January 2022 in spite of some 10% more of the population getting vaccinated from September through December of 2021.
A typical mandate example: in September 2021, Washington Governor Jay Inslee issued Emergency Proclamation 21-14.2, requiring COVID-19 vaccination for various groups of state workers. In the proclamation, the stated goal was, “WHEREAS, COVID-19 vaccines are effective in reducing infection and serious disease, and widespread vaccination is the primary means we have as a state to protect everyone… from COVID-19 infections.” That is, the stated goal was to reduce the number of infections.
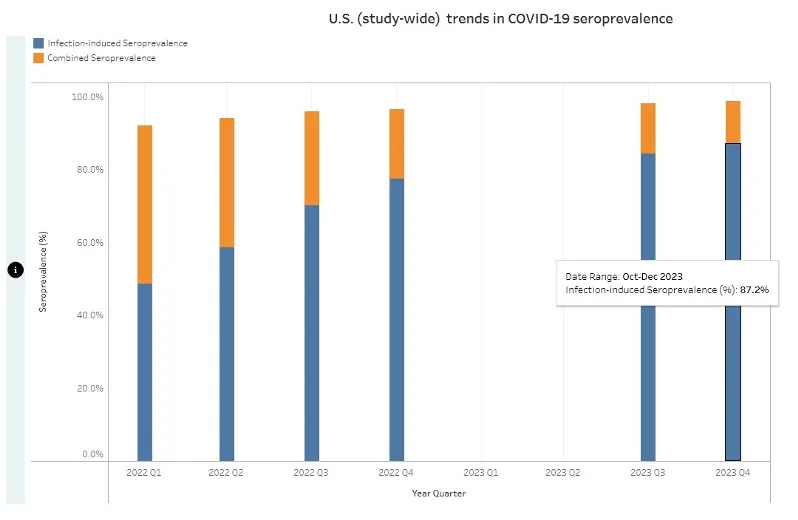
What the CDC recently reported (see chart below), however, is that by the end of 2023, cumulatively, at least 87% of Americans had anti-nucleocapsid antibodies to and thus had been infected with SARS-CoV-2, this in spite of the mammoth, protracted and booster-repeated vaccination campaign that led to about 90% of Americans taking the shots. My argument is that by making policies based on number of infections a higher priority than ones based on the more serious but less common consequences of both infections and policy damages, the proclaimed goal of the vaccine mandate to reduce spread failed in that 87% of Americans eventually became infected anyway.
In reality, neither vaccine immunity nor post-infection immunity were ever able fully to control the spread of the infection. On August 11th 2022 the CDC stated: “Receipt of a primary series alone, in the absence of being up to date with vaccination through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6). Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.” Public health pandemic measures that “wane over time” are very unlikely to be useful for control of infection spread, at least without very frequent and impractical revaccinations every few months.
Nevertheless, infection spread per se is not of consequence, because count of infections is not and should not have been the main priority of public health pandemic management. Rather, the consequences of the spread and the negative consequences of the policies invoked should have been the priorities. Our public health agencies chose to prioritise a failed policy of reducing the spread rather than reducing the mortality or the lockdown and school and business closure harms, which led to unnecessary and avoidable damage to millions of lives. We deserved better from our public health institutions.
Harvey Risch is a physician and a Professor Emeritus of Epidemiology at Yale School of Public Health and Yale School of Medicine. He is a Senior Scholar at Brownstone Institute, where this article was previously published.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“CDC has quietly admitted that all of the indignities of the COVID-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, and especially the vaccines;all of it failed to control the pandemic.”
Maybe it never needed controlling?
Just a deliberate test of mass public obedience!
Totally that, Dinger. It was exactly like a new-fangled Asch/Milgrim hybrid experiment. How far would people go if they knew they were ”just following orders”? How much damage and pain would they actually be responsible for if they could absolve themselves of blame because those instructions were coming from higher up? The teachers, the hospital/GP staff etc etc. Every country seemed to have different levels of tyranny and abuse, but a lack of compassion and humanity, whilst turning their backs on all evidence is what they all had in common. And as for replicating Asch, well….I think we all have our own lived experiences of the morons we’ve encountered, even friends and family, shamefully, who succumbed to the mania without question and went along with the hoax zombie-style, like something out of ‘Invasion of the Body-Snatchers’. The jury’s out on if there even was an actual ‘Covid’ virus, because you’ve still got people swearing blind they got some sort of unique symptoms or illness, but the data show that even if there was there were no excess deaths until the world went mental with the ‘response’, nothing from an illness in and of itself. Just a plain, old, unsexy flu-like… Read more »
Iatrogenesis. Injured or killed by the treatment received.
Nosocomial. Infection caught in the hospital.
Comorbidity. Aready very ill, something was bound to push them over the edge.
Three words we should all know by now.
Democide too!
Speaking of “just following orders”…
How about the vaccinators? The doctors, nurses, pharmacists and others who ‘followed orders’ and actually stuck the needles in arms, particularly under coercion, intimidation and mandates, as happened in Australia.
Now, according to Australian government statistics, over 70 million Covid-19 doses have been injected. How could this happen under coercion, intimidation and mandates?
Vaccinators – doctors, nurses, pharmacists and others – have a legal and ethical obligation to obtain voluntary informed consent for vaccination…it’s not possible to obtain ‘voluntary informed consent’ under coercion, intimidation and mandates…
So how did this happen? What happens when the public understands they didn’t actually give valid consent to this medical intervention, they were bullied into it.
What will this mean for the medical indemnity of the vaccinators?
Spot on. Went to an old company “do” the other night.
“Where’s Bob?” Someone asked.
“Oh he’s not coming he’s got Flu” was the reply.
“Not Covid then?”
“No“.
”How’s he know”
”Took the test”
And there my friends is a very large problem.
Never thought of that Mogs, funny how the flu went away while covid was needed! Maybe it was just the flu wrapped up in covid clothing to give a pandemic effect?
Well the DOD played its part. ‘countermeasures’ as a military term for, supposing it does exist, a bioweapon.
There was no pandemic.
“Covid case” is a nonsense phrase.
Hi ToF, it’s always worth repeating.
The pandemic was a mirage conjured by the excessive amount of testing using insanely sensitive tests. Ramping up the testing inevitably made it look like things were going to hell in a handcart.
What was referred to as a ‘case’ was nothing of the sort. The link between ‘case’ and coof-death was incredibly tenuous.
Some people did become quite ill, my partner included, it wasn’t pleasant but it was never the catastrophe it was made out to be.
I wonder if that will ever be acknowledged.
Thanks. I don’t think it will be widely publicly acknowledged in my lifetime.
“Admits to policy failures” is as good as it will get for now I think. I struggle to believe they were “failures”. The whole thing seems like theatre to me, and the CDC were I think playing a part.
If we’re incredibly lucky we might even get “Lessons will be learned”
Except they never are of course, but they always bring out the old trope anyway.
The most important lessons are not ones that the establishment wishes are learned. Importance of freedom of speech and the right to protest, bodily autonomy, proper checks required on the ever-expanding role of the state. The lesson the general public need to learn is that “conspiracy theories” are often true and you must always ask “cui bono” and remain very sceptical especially when you are told there is an “emergency” – and that the state cannot and must not try to “keep you safe” from everything.
Do you remember the date the WHO changed the definition, someone mentioned in 2019/20. But in the fog of all the information I for some reason thought they changed it around 2011 shortly after the Swine Flu failed psyop.
No I don’t remember. I thought it was in the very early days of covid, but it may have also changed after Swine Flu. I’ve tried to find the definition on the WHO website but it’s elusive. I’m sure someone has it archived somewhere. Possibly Collateral Global have a record of it. Someone did trawl all the old Lockdown Sceptics pages and archive them but the link I had to that no longer works.
The CDC is old hat. They are irrelevant now.
The WHO is where all the action is now.
The CDC was a useful tool for covid.
But if what you want to do is legislate for the whole world so that you can have the entire world population on a regular course of “vaccines” like livestock, then for that you need the WHO.
Well-said
Re: “…count of infections is not and should not have been the main priority of public health pandemic management”.
So how did this happen?
How did count of infections become the main priority of public health pandemic management?