“Unacceptable”: Calculating the Covid Vaccine Fatality Rate
Let’s clear up three points first:
- Forcing people to be injected, by coercion and threats, was a despicable intervention. Only an immoral mind could find it acceptable, and society has no shortage of immoral, ‘normal’ minds, as history shows.
- Covid vaccines have caused severe adverse effects and deaths. Only a prejudiced mind can deny this statement. They are neither safe nor as effective as initially claimed. There is considerable uncertainty about their true effectiveness (see here and here, for example).
- That any vaccine can cause death is not some novel discovery. The ultimate questions in science are quantitative, not qualitative: How often? What is the fatality rate of Covid vaccines? How does it compare with the fatality rate of, say, a flu vaccine?
TLDR:
- Fatality after a flu shot is extremely rare: one death per five million.
- Short-term fatality after Covid shots is many folds higher: dozens of deaths per one million. That’s unacceptable, or at least was unacceptable for any vaccine before 2021.
- We should also add long-term mortality, which is difficult to quantify. For instance, fatal arrhythmia two years later due to subclinical myocarditis. Is this tragic death an example or not? Who can tell? Unexpected death of young people had happened before, rarely.
- I do not think, however, that short-term Covid vaccine deaths have been a main contributor to excess mortality in the past two years. With some exceptions (here and here, for example), it is difficult to detect these deaths in country-level statistics.
Data sources
In the normal course of science, regulatory agencies would have set up well-designed cohort studies to estimate the fatality rate of Covid vaccines. That did not happen. They were too busy advertising the shots as ‘safe and effective’, so we have to derive estimates from other sources. That’s far from rigorous science but better than nothing.
I used several methods to estimate the likely range. Two sources allowed me to exclude implausible values. Other sources allowed me to narrow the range.
Below, I compute the rate as the number of deaths per 100,000, rather than per million, and consider the number of vaccinated people, not the number of doses.
Inference from serious adverse events
A landmark study, by a highly qualified research team, has estimated the rate of serious adverse events in the clinical trials of Pfizer and Moderna mRNA vaccines. The rate of such events was roughly 10-15 per 10,000 (100-150 per 100,000) above the rates in the placebo arms.
The rate of fatal events must be a fraction of the rate of serious adverse events, just as the number of patients who die in a hospital is a fraction of those who are hospitalised. What is that fraction in the case of Covid vaccines?
It is certainly small. Not 50%, not 30%, not 20%. I think it is no more than 10% of serious adverse events, and probably smaller.
We should therefore conclude that the fatality rate of Covid vaccines cannot be more than 15 per 100,000. The data on serious adverse events in the randomised trials (however problematic those trials might have been) allow us to exclude some implausibly high values. The short-term fatality rate of Covid vaccines is not 100 deaths per 100,000 nor 50 deaths per 100,000.
Inference from Israeli data
The first vaccination campaign in Israel took place at the beginning of 2021, concurrent to a Covid winter wave.
During that period (December 2020-March 2021) the Ministry of Health reported about 3,300 Covid deaths, whereas the Central Bureau of Statistics (CBS) later estimated only half as many excess deaths.
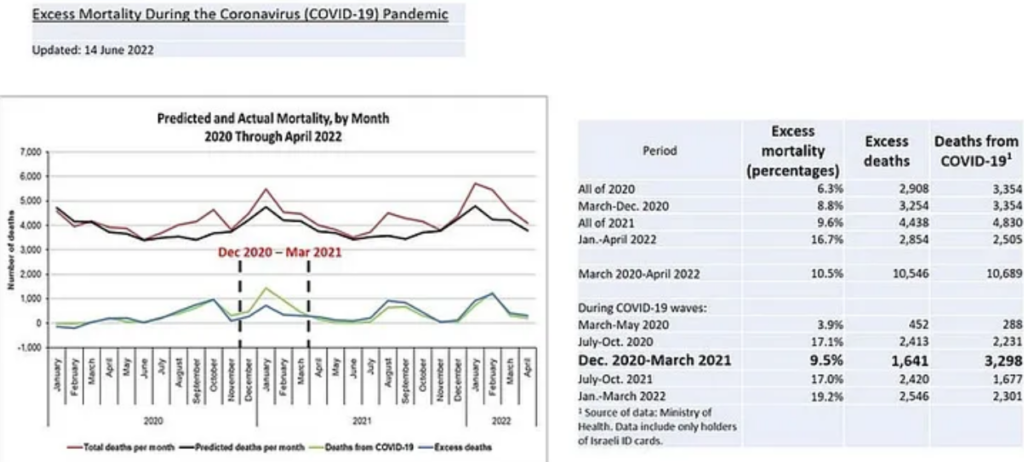
The CBS estimate of about 1,600 excess deaths in that period seems reasonable to me. I reached a similar number based on simple extension of a linear trend.
The striking difference between reported Covid deaths and excess deaths undermines vaccine efficacy studies from Israel. But it also sets an upper boundary on the short-term fatality rate of the Pfizer vaccine. Undoubtedly, much of the excess mortality at that time was Covid deaths, which means that only a few hundred could have been vaccine fatalities: perhaps 500 at most, among five million vaccinated residents.
That’s a rate of 10 per 100,000.
Rates that are much higher are incompatible with the number of excess deaths in Israel during the first vaccination campaign. For example, a rate of 50 per 100,000 implies 2,500 vaccine deaths when the total number of excess deaths was 1,600. Similarly, a rate of 20 per 100,000 implies 1,000 vaccine deaths out of 1,600 excess deaths. That’s implausible, too.
There is one caveat, however. The early post vaccination period is a high-risk period for contracting Covid and for death from Covid. Since the vaccination campaign coincided with a Covid wave, an unknown proportion of Covid deaths might have been vaccine-related. These deaths should be added to the numerator of the fatality rate.
Rough estimates from various countries
During 2021-2022, when Covid vaccines were injected into billions, I encountered counts of reported vaccine-related deaths from several countries. These reports were compiled by national registries, reflecting different cultures and different administrative structures. Some reports included the number of vaccinated people by some time point; for others I obtained estimates elsewhere.
I kept adding lines of data to an Excel file. At that time, I did not envision publishing an article, so I did not keep a record of the data source, the date, or a link to a website. I simply wanted to know the truth, which authorities were trying to hide. The numbers I obtained are ‘crude’ — in any sense of the word you would like.
Here are my data, without much editing:
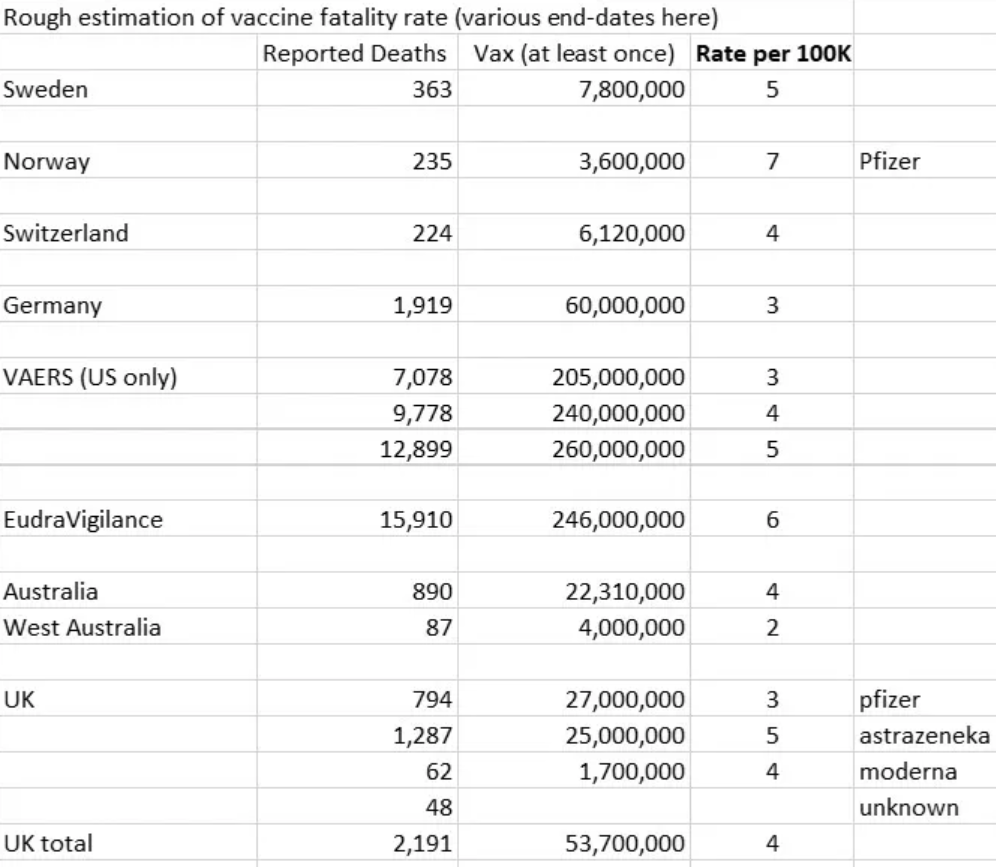
Can we still learn something from such raw data? I think we can, relying on heuristic arguments.
Reports from different countries and different cultures have returned a narrow range of the fatality rate (2-7 deaths per 100,000). They cannot be wrong by a similarly large factor (e.g. 10, 20, 40). Otherwise, we would have to assume, for example, that Sweden and the U.S. share the same huge under-reporting bias (e.g. only 10% of vaccine deaths are reported in each country).
Stated differently: to assume a large error, we have to assume that data from different countries are not only extremely bad but were also somehow ‘standardised’ to be just as extremely bad – everywhere. No exception.
I would not make such an assumption. The rates from different countries are likely underestimates of the truth, but the correction factor may be two to four at most. Not 40, not 20. Not 10. Many deaths after a vaccine shot are unexpected and not easily ignored by medical personnel. I think that a significant proportion of these deaths has been reported, even in the Covid era, when biases prevailed.
In the table below, I summarised the data as follows:
First, when millions are vaccinated, some reported deaths are coincidental. To be conservative (favouring the vaccines), I assumed that only 75% of reported deaths were vaccine-related.
Second, I allowed for an under-reporting factor (URF) of two (only half is reported), three (only one-third is reported), and four (only one-quarter is reported).
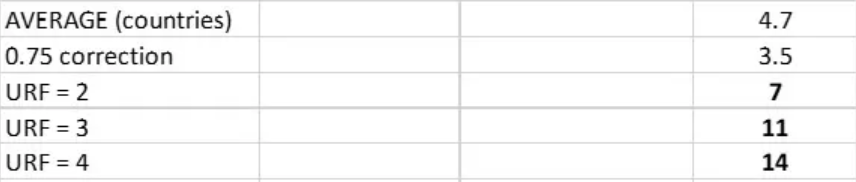
Extending the 7-14 range somewhat, in both directions, we may assume that the fatality rate is somewhere between 5 and 15 deaths per 100,000. The upper limit is in line with the number I deduced from the rate of serious adverse events.
In the U.S, these rates imply at least 13,000 short-term vaccine fatalities and possibly three times as many (almost 40,000 deaths). Statistically, few of these people would have died from Covid.
Booster
Many of those who completed the first vaccination protocol (two doses a few weeks apart) received a third (booster) dose several months later. There were booster-associated deaths (see here and here), and they add to the count of vaccine fatalities, probably doubling the overall short-term fatality rate.
Some insight, albeit not scientific, may also be gained from what are sometimes labeled ‘sentinel events‘.
Back in 2021, I was following a news outlet in my state and noticed a cluster of five unexpected deaths of relatively young people over a short period (November 4th through December 4th). Unexpected deaths are not usually reported unless the deceased is a public figure in some sense, which was the case here. The deceased worked in professions that may be called ‘protective services’ (see here, here, here, here, and here). In one case, “sources” reportedly said it was Covid. The circumstances of other deaths remained obscure.
Sometimes, the general descriptor was “in the line of duty”, which is non-specific, and elsewhere included Covid death (see here, for example).
Did they all die from Covid? Suddenly? That’s unlikely. Furthermore, deaths from Covid of police officers were highlighted in the local media, not hidden (see here, here, and here).
Were all of them vaccinated? I do not know (though it is likely, especially in those professions).
If they were vaccinated, was the death vaccine-related in any case? I do not know.
But I do know that the time period roughly coincided with the timing of a booster dose. I also know that a cluster of such deaths in one month is highly unlikely, statistically, in the absence of a time-dependent shared cause.
From what I could find, there may be 40,000 people or so in such professions in my state. If these were booster-related deaths, the rate is in line with the estimates.
Booster deaths or not, we do not expect to hear about five unexpected deaths, in one month, of relatively young people in occupations that require excellent health status. I am not aware of any investigative report about this unexplained cluster of deaths.
Summary
Fatality after a flu shot is extremely rare: one death per five million.
Short-term fatality after Covid shots is many folds higher: dozens of deaths per one million. That’s unacceptable, or at least was unacceptable for any vaccine before 2021.
What about long-term consequences, fatal and non-fatal? Will we be able to estimate the rates in a decade or two? How would we know, for example, if a future Covid death was caused by changes in natural immunity? How would we know if a sudden death was caused by subclinical myocarditis? How would we know if an auto-immune disease was triggered by Covid vaccine?
This is not going to be an easy task.
There had been good reasons, before the Covid era, for not rushing a new drug, or a new vaccine, into the market. We have learned the lesson the hard way, or have we?
Dr. Eyal Shahar is Professor Emeritus of Public Health at the University of Arizona. This article first appeared on Medium.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Yeah whatever. Excess deaths in every country exploded post the jabs. 100 K dead in the UK from the Stabs out of 40-50 million jabbed and that is just the start. Millions injured. Injury and death rate is 2%or more, probably closer to 10% if you add in ‘minor’ injuries that go away (maybe they are resolved, maybe not). Longer term – cancers, neurological issues, heart problems etc. All blamed on bacon, climate-thingy, transphobia. 10% injury and death rate in the longer term from the Quackcines.
Rona was the greatest medical nazism and debacle in history. Simple as that. Millions dead and injured worldwide. You can parse and vomit all the made up data and made up analysis you want. You can quote from corrupt fake fact checkers until diarrhea pours out your nose. My lying eyes and the world of the 5 senses tell me what really happened. The quackcines are poisons and not a single Rona-tard I asked, who happily jabbed 3-5 x can name or spell 3 ingredients or explain how it all works. ‘Science’ they moan. Stupid I reply.
Indeed.
At this point I fear that most people have decided consciously or subconsciously that whatever happens, whatever shocking information emerges, they don’t want to know, they want to move on and pretend it never happened.
I agree, but I’ll wager there’s a large minority that will never let it go! The families of those affected and all those with a true sense of morality and justice!
Not to mention the massive majority that don’t want to get any where near another one of those jabs. That’s real too.
👍👍
Yes I think they know they were had
Indeed. And another side effect could be that they have lost confidence in other products on offer. Thus the “health service” has lost it’s reputation.
And, this might get worse before it gets better! The long term effects of the dna vaccine manipulation are totally unknown, this could be a generation killer!
Indeed
They will keep the issue alive long enough for the historians to properly record the folly and evil
I wish I could like this comment several times over.
We don’t need more stats.
We can SEE the sudden deaths from heart attack and stroke and the turbo cancer. We all know people who have had chronic conditions appear or worsen since they took the poison.
And yet us who never touched the death jabs….we’re fine.
Here here. I can’t contribute to this ‘cockup, incompetence’ nonsense anymore. Sick of it and being called a conspiracy theorist by a so called sceptical news outlet is tiresome. Listening to London Calling with Team Tobes take on the totalitarianism is painful, same the the DS podcast. Will redirect funds to Team James instead. #TeamTruth
Important paper just out. A scientific investigation looking at the alleged protection of the clot shots from severe illness and death. Conclusion;
”The widely accepted medical narrative today, as if the booster doses of the mRNA vaccines prevent severe illness and deaths despite their failure to protect against infections, lacks scientific support. It is more likely that this proclaimed efficacy against severe illness and deaths is merely a wishful myth, which has no empirically grounded evidence. We therefore openly call for an immediate, even if temporary cessation of the vaccination campaign until real evidence is available, especially considering the critical safety signals, which seem to be downplayed unjustifiably in the medical and scientific discourse.”
https://www.jpands.org/vol28no1/ophir.pdf
Accompanying video ( 13mins ) of the lead author talking about his findings.
https://www.youtube.com/watch?v=ZbTwoTMBB6Q&ab_channel=YaakovOphir%2CPhD%7C%D7%93%22%D7%A8%D7%99%D7%A2%D7%A7%D7%91%D7%90%D7%95%D7%A4%D7%99%D7%A8
Very, very good.
It is very obvious from this analysis and stunning how fraudulent the Pfizer/Moderna trial results were and/or have been interpreted and promoted and how uselessand dangerous the gene therapies really were and are.
The other ones discussed and their main conclusion as cited by you only delve into the boosters though (outside of the small healthy vaccinee effect).
Importantly, these latest findings then fly in the face of the argument that the gene therapies were ever/are currently required to protect the elderly from dying of Covid. It amazes me that we still get people on this site ( I think Noah Carl is one such person ) or the likes of Dr Vinay Prasad, John Campbell, for example, who still maintain these shots offer protection to those deemed at high risk in society, or that the jabs are responsible for saving a significant amount of elderly people’s lives. This analysis contradicts that notion. These injectables benefit nobody, especially when a risk/benefit analysis is done taking into account the proven terrible safety profile and the suppression of existing early treatments and antibiotics. Completely unnecessary for all cohorts.
I think John Campbell has adjusted his point of view quite a lot recently, if you read between the lines (bearing in mind that his YT channel is still live). Anyway, I agree with your position.
The injectables benefit only the manufacturers’ bottom lines. And as these manufacturers have no liability for the consequences of their injectables why should they care? Our error is to believe the manufacturers work to the moral norms usually expected in civilised society.
“ We have learned the lesson the hard way, or have we?”: It depends what you mean by we, but in your trade you should have access to relevant historic records. It looks as if some of them like to ignore much of them, and grabbed hold of the idea that “emergencies” can be used to justify high levels of risk associated with new drugs.
From a private view, I’m glad I said something like “no, not yet; I’ll wait and see if it becomes an established product”. Of course, in effect, it has not become established as a worthwhile thing in relation to the alleged benefit.
I used to claim that the Pfizers, Modernas et al were using billions of people as free lab rats.
Now I know they weren’t looking for lab rats, because they weren’t interested in actually testing anything.
Well, in reality yes. They used the global population wide experiment to get their new technology globally approved, paving the way to migrate all vaccines to their new proprietary technology.
So billions were lab rats, not for effectiveness or safety testing purposes, but for much more mundane bureaucratic expediency purposes.
Indeed. Getting their mates in governments to spend our money on them. We and our children foot the bill. It’s genius.
Exactly so Stewart…getting people to accept mRNA unproven, dodgy, dangerous technology as something else…..as if it been ‘proven’ a safe technology when it couldn’t be further from the truth…. If you can access Twitter Thomas Renz has a good thread about mRNA jabs for cattle in the USA….. https://twitter.com/RenzTom/status/1642229969555259395 BREAKING NEWS: the lobbyists for the cattleman and pork associations in several states have CONFIRMED they WILL be using mRNA vaccines in pigs and cows THIS MONTH. WE MUST SUPPORT #Missouri #HB1169. It is LITERALLY the ONLY chance we have to prevent this… NO ONE knows the the impacts of doing this but we are all potentially facing the risk of being a #DiedSuddenly if we don’t stop this…. And let’s not forget the UK Government and Moderna … Moderna, Inc. has finalised a strategic partnership with the UK government to establish a state-of-the-art mRNA vaccine research, development, and manufacturing facility in the UK. This milestone follows the agreement in principle between Moderna and the UK Government, announced in June 2022. With Moderna investing over a billion pounds….. The Moderna Innovation and Technology Centre (MITC) is intended to provide access to a UK-made supply of COVID-19 jabs. It also has potential to develop… Read more »
LOL, I was just reading that earlier. I’ll provide a link to his ‘stack to supplement your link…Gawd, if it’s not bloody insects we’ll soon be on the lookout for more nasties in our food! 😮 ”The fact that food can be altered to act as a vaccine is not disputable. Which foods and in what ways is more of a question. It is claimed that beef, pork, etc. cannot transfer vaccination from the meat to a the consumer of the meat. At initial glance that would make sense (cow DNA and people DNA is quite different and an mRNA designed for cows would probably not be able to transfer directly to people), but that is NOT the whole story. You have to remember that the additives in the mRNA vaccines are by no means “proven safe” and we don’t even actually know what all is in these shots. The Lipid NanoParticles (LNPs) appear to be a problem and there have been numerous reports of “other things” some scientists have found in the jabs when they examined them. Ultimately the mRNA jabs still have not undergone long-term testing because long-term testing can take 10-20 years and they have not existed… Read more »
I hadn’t even stopped to think about livestock.
I just had a quick look at the recommended vaccines for cows and chicken. It’s a long list. More than a dozen for chicken in just one year and more for cows.
Considering there are over 30 billion chicken in the world and over a billion cows I’m just beginning to understand just how huge the vaccine industry is. It’s mind boggling.
Well the jab in the arm didn’t work out as well as they hoped..so they have to think of another way to get the poison into the population!
https://dailyclout.io/eat-your-vaccines-mrna-gene-therapy-is-coming-to-the-food-supply-this-month/
TPTB appear to be in damage control mode currently. Throwing AZ under the bus for clotting to distract from the affects of the other two.
The MHRA and the JCVI need to be completely overhauled and there should be criminal charges applied, but unfortunately it simply won’t happen. The new CMO taking over from Vallance is the continuity big pharma candidate so nothing will change.
I just wish governments would have been as cavalier about “covid” deaths as they are now about jab deaths.
If they had been, they could have avoided murdering thousands of people who died from a jab they were forced to take and never needed.
Plausible. But so is the recent Rasmussen poll.
https://stevekirsch.substack.com/p/vax-deaths-covid-deaths-according
And the latter indicates that the underreporting/ignorance/deceit factor is just far larger everywhere than assumed here.
I learned of a story yesterday that confirmed it: a friend in Germany is always sick with breathing difficulties since being poisoned with the goo. She now has had pneumonia diagnosed and was courageous enough to tell her story and blame the goo for it in front of her doctor.
The doctor totally freaked out and showed the patient the door instead of taking her serious, let alone reporting it.
Obviously, they see personal liability issues arising and shun the unpaid reporting work in such cases.
Even more obviously, he and most of the goo-ing doctors everywhere are just sc*m.
They are stupid, ignorant tools as shown by the fact that they are the only idiots in the entire population that still pretend surgical masks are going to protect them from a virus.
It’s very, very difficult to retain any respect for these people.
Interesting piece. I suspect the author is right. The level of deaths from the vaxx hovers around the level of noise in the data, making it hard to isolate it. This is why the anecdotal becomes relatively more important.
Good summary of the earlier scams.
https://www.globalresearch.ca/stay-home-save-lives-uncovering-covid-deception/5814448
Absolute bottom line? Do not trust Big Pharma!
When I worked for a pharmaceutical company (which was eventually engulfed first by another company and then by Pfizer) there were very strict internal rules concerning ongoing trials and monitoring of the data of our products in the healthcare market. We had very strict ‘chain of evidence’ rules for the forms and triple data entry of trial data for statistical processing. We generated reports about how often the data entry folk made mistakes (initially detected by the three entries for any one set of data not being the same) and had random sampling of 1% of completed data entry for an additional check. It was a major pain in the arse when we once found an error in the data entry in that 1%. It was eventually put down to a mis-reading of written numerals 1 and 7 on a particular set of submission forms (doctors’ hand-writing). We took being able to prove our trials were ‘kosher’ very seriously. But our new masters found the site where I worked to be not cost-effective (quite possibly for other reasons) and got rid of us. I find it astonishing that there is apparently no decent trial data available since injecting these new… Read more »
Some of the death estimates that are being claimed elsewhere (e.g. Rancourt) do seem to be too high, just considering highly-vaxxed Sweden, but since we’re emerging from what was supposedly a deadly pandemic that particularly affected those close to death anyway, there should be a substantial mortality deficit at the moment. We’re not seeing a mortality deficit anywhere, so vax fatalities may well exceed “excess deaths” unless those excess death figures allow for that underlying expected mortality deficit. The estimates in this article may be too low.
This is my first post here. Been reading the DS since it started up and finally subscribed, seeing as it’s kept me sane for the last couple of years. This is a really good article, very simple explanations. Does anyone know how to contact the editors of the DS to submit ideas?
Hiya JB, and welcome. I don’t know if there is a different way, but if you select the ‘daily-round up’ from the home page, at the bottom of the items listed in the ‘round-up’ there’s this “If you have any tips for inclusion in the round-up, email us here”…I’ve used it to contact them, for instance when I was locked out of my account, so I think you can use it for most things……hope that helps….
10 Jan 2023 Secretary Austin rescinded the Aug. 24, 2021 memorandum mandating that members of the Armed Forces under DoD authority be vaccinated against COVID-19, and the memorandum of Nov. 30, 2021, pertaining to the vaccination of National Guard and Reserve personnel.
So there is a well defined and sizeable group out there, in theory 100% of whom had all mandated vaccines over a 14/15 month period.
I don’t know how far freedom of information extends into the U.S. Military Health Service but there will be detailed medical records for these military personnel.
So it should be possible to come up with a detailed report regarding covid 19 adverse effects using that data?
The legal class action against Astra Zeneca, where 81 patients died and 364 suffered severe reactions, should keep vaccine adverse effects in the public eye. ‘Peter Todd, a consultant solicitor with Scott-Moncrieff & Associates, one of two lawyers handling claims, told The BMJ that the complications included stroke, heart failure, and leg amputations. He said the technology involved in the AstraZeneca vaccine was “risky.” Even though the legal claim is against AstraZeneca, the UK taxpayer will have to pay any compensation awarded, under a legal indemnity that the government gave the company early in the pandemic. In response to a freedom of information request, NHS Business Services, which operates the vaccine damage scheme, revealed that by 6 March 2023 the scheme had received 4017 claims relating to a covid-19 vaccine. Of those which had been dealt with, 622 concerned the AstraZeneca vaccine, 348 the Pfizer, and 43 the Moderna vaccine. Of the 4017 claims, 334 were for a death. Sarah Moore, a partner in the Hausfeld law firm, whose clients are also taking legal action, said the maximum £120 000 payment from the scheme was “nothing” in cases where the person who was injured or died was a breadwinner. “Many were parents and… Read more »
That’s what the DMED scandal was about, the US military has a unified medical system and its reporting database showed the adverse events https://stevekirsch.substack.com/p/this-medical-data-from-the-us-dod
Thanks for that, and even more data available now.
I don’t think any cover up will work in the U.S.
We shall see.
It wouldn’t make sense to try to jab everybody multiple times
unless the jabs did serious harm.
But jabs that killed quickly would clearly have a low take-up rate after the first few months
Therefore the jabs are designed to do harm over a long period, and it is far too early to have any idea about exactly how damaging they are.
This article is based on reported deaths, and in my view using this unreliable number makes this analysis nul and void.
The best way forward would be to do analysis of cohorts of vaccinated and unvaccinated people. Looking at deaths and other side-effects. This should be an ongoing study, picking up long-term side effects as these happen.
I know nine people who ‘had a change in their health’ following the jabs..however not one of them attributes it to the vaccine.
How can you trust the stats when people are in denial that they’ve been harmed?
Excuse me but are we assuming that the “Covid” deaths were from or with Covid here? Bearing in mind 95% of people who died with Covid on their death certificates had between 2 and 3 other ailments? I.E. only 5% died OF Covid. This would surely put the death jabs into an even worse light.