Sharp Drop in Treatment for Blood Infections Due to Lockdown Causes Hundreds of Avoidable Deaths
Escherichia coli – E. coli for short – is a bacterium with two faces. Some strains produce toxins that cause gastrointestinal disease. Set these aside. We’re concerned with the other strains that live innocuously in the colon. They’re among the most abundant gut bacteria and only cause trouble if they reach other body sites.
This happens if the gut contents leak during surgery, for example, or via a ruptured appendix. More commonly, particularly in women, gut E. coli reach the urinary tract and swim upwards, causing UTIs (urinary tract infections). Some strains are especially adept swimmers; five or six ‘uropathogenic’ lineages account for half of all UTIs.
In total, E. coli causes 80% of all UTIs, with 150 million cases annually worldwide. Most are painful but self-limiting ‘cystitis’, reaching no higher than the bladder. These used to be treated with trimethoprim. Nowadays, owing to trimethoprim resistance, nitrofurantoin is preferred. A few reach the kidneys and, worse, then spill into the bloodstream. That’s bacteraemia – bacteria in the blood – which can trigger life-threatening sepsis.
E. coli accounted for a third of all U.K. bacteraemias in fiscal year 2019-20, with a tally of 43,395 cases, mostly in the elderly. Hospitals in England are obliged to report these, so numbers should be robust. UTI ‘overspill’ accounts for at least half; gut leakage for a quarter. Most UTI-origin cases develop in the community and enter hospital through A&E.
Around 18% of E. coli bacteraemia patients die in the U.K. This rate roughly doubles if treatment is inadequate, usually because the E. coli strain was resistant to the first antibiotic given. (The patient must be treated immediately but it takes two days for the lab to get results, creating a window for error.) Mortality must be similarly high among untreated bacteraemias. Keefer, at the end of the pre-antibiotic era, found 35% deaths.
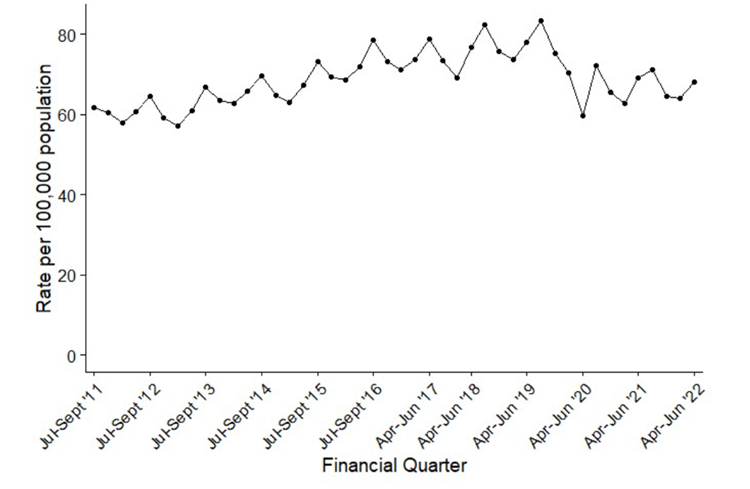
Right, that’s the background. Now, look at case incidence for England (figure 1). Three points stand out: 1) a long upward trend to 2019-20; 2) summer peaks, never properly explained and 3) a big step down at the start of the Covid pandemic. It hasn’t gone up again.
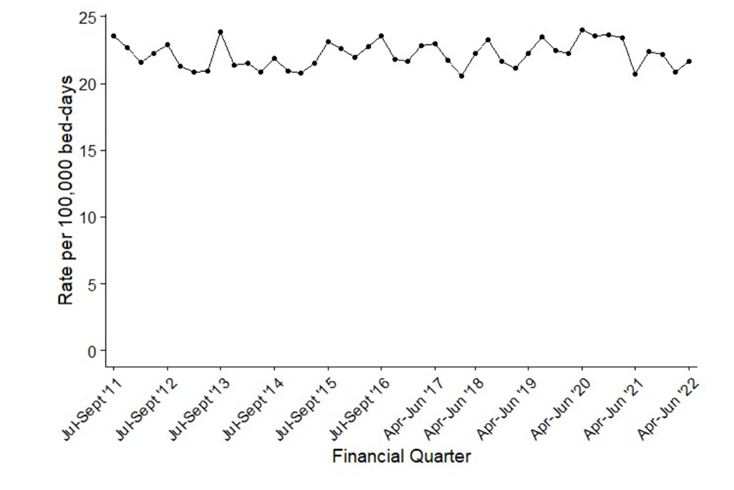
This step isn’t apparent – with a caveat below – for the subset of hospital-onset E. coli bacteraemias (figure 2), or for Klebsiella (not shown), which is related to E. coli, but is largely a nosocomial (hospital-caught) pathogen.
Why?
Five possible explanations can be dismissed:
- COVID restrictions suppressed them. This lacks plausibility. E. coli bacteraemias involve the patient’s own gut flora. Lockdowns, social distancing, masks etc. don’t alter proximity to our own gut. Moreover, case numbers didn’t rebound after restrictions eased over a year ago.
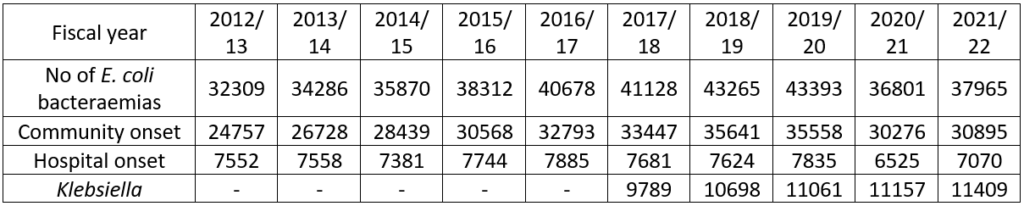
- A denominator issue. This is unlikely for figure 1, where rates are expressed per 100,000 population, and a delve into the raw numbers (table below) shows exactly the same pattern. There is an issue for figure 2’s hospital-onset cases, which are reported per 100,000 occupied bed days. Here, the raw case numbers are flat from 2012/13 to 2019/20, with a 16% drop in 2020/21 and a partial rebound in 2021/22, perhaps reflecting a different case mix through the pandemic or altered hospital occupancy. Hospital-onset cases are often gut-surgery-related, not urinary.
- Hospitals are failing to report cases. This can’t be wholly dismissed. But, were it the major factor, one would expect the tally of community-onset cases to show the same rebound in 2021-22 as for hospital-onset cases. It doesn’t. What is more, reported Klebsiella bacteraemias rose continuously to 2021-22.
- SARS-CoV-2 killed the patients who develop E. coli bacteraemias. Some erstwhile PHE colleagues believed this in 2020, and it may be part of the story. But Covid deaths are fewer now, and new people are reaching decrepitude, making them vulnerable to E. coli. So, numbers should have bounced back, but haven’t.
- The change from trimethoprim to nitrofurantoin reduced the number of UTIs progressing to bacteraemia. It would be nice if this was true, but it isn’t. The switch in prescribing was progressive, largely from 2016 to early 2019. It can’t explain a much later and steeper fall in bacteraemias.
So, we’re left with the likely explanation: that community patients whose UTIs ‘go bad’, leading to potentially fatal bacteraemia, aren’t presenting at A&E. Maybe they are not even receiving treatment for the underlying UTIs in the first place. A drop of 60-70% in UTI diagnoses was asserted early in the pandemic, with only a partial ‘recovery’ by October 2020. Formal publication and extension of these important data is still awaited.
Next, consider two strands of anecdotal evidence. First, Carl Heneghan stresses how easily a UTI is missed in 92-year-old Mrs Jones who – as so often with the very elderly – lacks typical symptoms. Rather, she “is a little confused and a bit wobbly on her feet, though all her observations are normal”.
She’d be even harder to diagnose via a telephone consultation, should she be able to book one. Which brings us, secondly, to the ex-wife of a prominent Cabinet Minister calling her GP apropos a respiratory tract infection.
After 47 attempts to get past the ‘engaged’ tone (my phone logged them), I finally got through to a recorded message about how busy they were, and I was placed in a queue. I actually felt grateful.
I waited a further 40 minutes before the receptionist finally answered, only to be told – you guessed it – that no appointments were available.
On Tuesday, the infection was much worse. I tried again. This time it took 45 minutes to get through. Again, no appointments were available. The receptionist suggested emailing.
It’d be no easier for a UTI. And it’d be harder if, unlike Sarah Vine, you are 92 years old, a little confused and wobbly on your feet. It’d be tempting to give up. Numerous missed UTIs and consequent community-onset bacteraemia seem very likely.
As has been widely flagged, the U.K. is persistently recording 10-15% excess mortality. Unusually large numbers of deaths are occurring at home. My view is that these deaths overwhelmingly comprise groups who didn’t or couldn’t access medical attention over the past two and a half years. At present cardiac deaths are prominent. Still to come is a large slab of deaths from cancers that would have been treatable had they been diagnosed in 2020, but which were diagnosed late.
But somewhere, hidden among the total, is a slice of my missing community-onset E. coli bacteraemias. A mortality rate of 35%, as in the pre-antibiotic era, would predict 1,750 deaths among missing 5,000 patients, half of them preventable with adequate antibiotics. So, a little under a thousand annually. But, it’ll be significantly higher if, as is very likely, more untreated ascending UTIs has led to more undetected bacteraemias than before the pandemic.
Dr. David Livermore is Professor of Medical Microbiology at the University of East Anglia.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
6. A growing distrust of the medical and pharmaceutical worlds has caused a massive drop in attendance, across the board.
Unfortunately, I believe this sort of thing was deliberately planned for. TPTB knew from the outset that shutting down the NHS for two years would lead to excess mortality figures and also knew that their ready made excuse – it was the covid wot done it – would provide the perfect cover.
I am certain this is just the start and matters are sure to get much worse. It’s genocide alright.
Evil unbounded.
My partners daughter, still in her 20’s, got Sepsis during the Pandemic. She was working as a care worker over near Heathrow. She delayed going to hospital because she was worrying about her elderly charge. But when she herself became bedridden and feverish and the elderly woman she was supposed to be looking after, ended up looking after her, an ambulance was called (incidentally the agency she was working for were awful and treated her illness like it was a terrible inconvenience). At Ashford hospital (I think it was) she was treated like a Lepper. Questioned aggressively why she wasn’t at her home address she was basically told off and told she almost certainly had Covid and should leave the hospital immediately. She returned to my partners house in Wimbledon but was clearly feverish and we rushed her to Kingston hospital by car. The A&E doctor there was far more switched on, diagnosed sepsis, declared loudly to the nurses “this young lady is not to leave this hospital” and generally ensured she got full attention and treatment. She was in hospital for a further 4 days before being discharged.
save the NHS indeed.
save the NHS indeed.
Oh yeah. I’ve got a horrible NHS story that’s happened today. Nothing more to add: only that it’s a small consolation that not once did I go out and clap.
The NHS is a disgrace to a civilised so-called society.
The NHS is a disgrace. Period.
Around 10 years ago, whilst at Oxford, my son got acute appendicitis. Unfortunately, he was admitted to Addenbrookes Hospital around mid-day on a Friday. An emergency appendectomy was scheduled for that afternoon.
It was delayed; then delayed again. And mid-afternoon on Saturday his appendix ruptured.
The hospital had de-prioritised him – apparently a child needing teeth extractions was more important because he/she was distressed.
They pumped him full of antibiotics and were intending to delay the appendectomy until the Sunday, until we kicked up merry hell and they finally operated at around midnight on the Saturday.
I lodged an official complaint and they – eventually – admitted that they had failed to follow their own procedures for prioritising patients and had exceeded the time-limit for patients requiring an emergency, potentially life-threatening, operation.
The NHS has not been fit for purpose for a very, very long time.
Interesting article.
To add to the mix, the effect of repeated jabs as immunosuppressants would suggest more, not less cases of E. coli sepsis. Secondly, I assume very few autopsies are being performed, as in Australia. Therefore, in patients with multiple pathology, the chance of error on the death certificate is high.
Added to that, a recent positive Covid test leads to that being the certified cause of death, even if it is actually E. coli septicaemia.
Why are there so many UTIs?
In ladies the close proximity of the outlets for urine and faeces, compared to men, doesn’t help. The other major issue, according to my ex-nurse wife ifs a lack or personal hygiene. Ugghh 😲
makes sense and could explain some of the excess deaths.
Excuse the simplistic question but if Sarah Vine’s GP is notseeing patients, like so many other GPs, how come they’re “very busy”?