Bangladesh Mask Study Results Are Consistent With No Effect
Approximately one year ago, I wrote about the Bangladesh mask study – the only randomised control trial of community masking since the start of the pandemic. (The well-known Danish study examined the effect of masking on the wearer; not the effect of community masking on community-level outcomes.)
While the Bangladesh study did find significant differences between the treatment and control arms, I described it as a “missed opportunity”. That’s because it wasn’t an RCT of mask-wearing per se, but rather of mask promotion campaigns. And the latter may influence transmission through mechanisms other than mask-wearing – such as by changing people’s behaviour.
Now there’s a new critique out claiming the study’s original conclusions may be wrong. It’s a bit technical – let me explain.
In a typical RCT: 100 patients get the drug, another 100 get a placebo, and you compare how many in each group get sick. But the Bangladesh study had a much more complex design – as shown in the figure below.
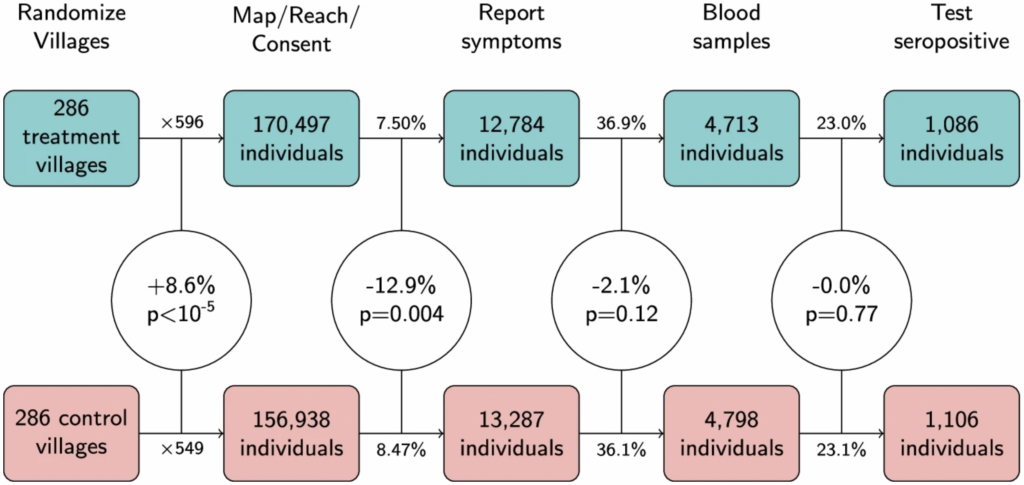
Headings across the top represent different stages of the experiment: first villages were randomized; then individuals within those villages were sought for consent; then they reported their symptoms etc.
The main thing to notice is that there was a statistically significant 8.6% difference between the treatment and control arms in the number of people who agreed to take part – 170,497 versus 156,938. (For those well-versed in stats, the corresponding p-value was less than 0.00001.) This isn’t supposed to happen in an RCT.
As noted by Maria Chikina and colleagues, who wrote the critique, this difference arose because the staff who went out to the villages and sought people’s consent were unblinded (i.e., they knew whether they were visiting a treatment or a control village). As a consequence, those in the treatment arm behaved slightly differently from those in the control arm.
Crucially, the 8.6% difference is as large as the main result of the original study: seroprevalence in the treatment arm was 8.7% lower than in the control arm. This means the main result could be due to factors other than the experimental treatment – even though the study was technically an RCT.
In fact, when Chikina and colleagues calculated the difference in seroprevalence measured as a count rather than as a rate – i.e., by comparing the absolute number of cases in each arm, while ignoring the denominator – they found it was only 1.8%. And you could argue this is the “correct” way to calculate the difference, given that randomisation of the denominators failed.
Overall, the new critique doesn’t prove the original conclusions are wrong. But it does show the data are consistent with mask promotion campaigns having had zero causal influence on the outcome variables.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Thanks for this. Only a nutjob conspiracy theorist could have predicted masks didn’t work.
I’m one of them – still am. In fact I think the virus is to. I had the most awful mild infection of the covid plague. So infected the LFT line was black let alone red. Had this unbelievably mild fever and horrifically mild sniffles. But amazingly the two unmasked and unvaccinated girls of the house did not get infected. Only a nutjob virus would ignore them.
Sex discrimination perhaps?
Did not think of that – virus needs cancelling. I’ll get PayPal on to it.
To my mind there has always been a strong whiff of opportunism, and the “something must be done” attitude. The belief that they could do any good for limiting the flow of such tiny compounds is for the birds. Especially so for the junk that has been sold to the public. Remember, if anyone had the ability to read the tiny labels on many of the products on sale (ideally using a magnifying glass), they would observe that they were not proper “medical masks” at all. Of course, such labels were there to avoid being done under trading standards. You could buy them, and the trader would be immune against prosecution under trading standards legislation.
So, it’s no surprise that there was no valid evidence of their efficacy – but hats off to those who have apparently spent a bit of time on academic work on the topic! Perhaps they even got paid for it.
Masks were promoted by the behavioural science subcommittee of SAGE to increase the public perception of fear. No other reason for them.
And that has really stuck with some people, hasn’t it? I was horrified when I bumped into two elderly friends in the doctors surgery yesterday, to see they were both double masked, the inner mask looking very tight and restrictive as well, almost like a bandage. I don’t say anything as they are gentle and frightened souls, and I am never going to change their minds, but it’s just so sad. Incidentally all of us waiting in the queue for prescriptions (nobody else was masked, including the receptionist) discussed loudly the fact that, as usual, there were no patients waiting to be seen – there never are – and how appalling the NHS has become. All the fat women hiding in the back couldn’t have failed to hear our loud complaints!
‘Bangladesh Mask Study Results Are Consistent With No Effect’
Yes we know – because since anything other than total face covering, tight fitting, respirator masks with filters cannot stop viruses, the ‘study’ could not truly yield any other result.
Masks were never about controlling the spread of any pathogen, all about compliance.