ONS Data Suggest Vaccine Effectiveness Against Death Has Been Overestimated
I was recently involved in a fairly lively discussion with a group of acquaintances, just about all in their 40s. Most of them had recently had bouts of Covid of varying levels of severity, yet they all seemed to think they’d been lucky that they’d dodged a bullet and that without the protection of their multiple vaccines they wouldn’t all be here to tell their tales. I thought their faith was misplaced and that their recoveries owed much more to their general health than any vaccination. The fact that the discussion occurred in a gym where they all regularly exercise their relatively healthy, lean bodies, made the whole conversation even more bizarre. I suspected they wouldn’t be interested but for my own peace of mind I thought I’d go away and see if the data supported their view or mine.
However, finding real-world data on vaccine efficacy is increasingly difficult. In recent months the UKHSA, ONS and NHS have stopped releasing real-world data on Covid cases, hospitalisations and deaths by vaccination status. This makes it effectively impossible to see if claims for vaccine efficacy turn out to be substantiated.
In previous articles I’ve used data from UKHSA and ONS to question both the protection vaccines afford against infection and against death. However, the data I’d used in these pieces only covered a relatively short time period. I wanted to see if I could find data covering the impact of vaccines on 40-somethings right through the vaccination period.
I thought a good place to start would be the fascinating paper by Professor Norman Fenton, Martin Neil, Clare Craig, Joel Smalley and colleagues, “Official mortality data for England suggest systematic miscategorisation of vaccine status and uncertain effectiveness of COVID-19 vaccination“, which delivers a devastating critique of so much of the official narrative. Could this give me any pointers? It led me to a report, “Deaths by Vaccination Status“, produced by the ONS. Tucked away in the dataset I found a set of data, Table 9, which seemed to have just what I was looking for: data on deaths by age cohort in the weeks following vaccination. Using these data I was able to compare deaths of vaccinated people in the different age cohorts, week by week in each of the sequential weeks from their last vaccination.
Because the report analysed data on a week by week basis from vaccination it effectively created something of a control group. People getting vaccinated were supposed to be clear of the virus for at least four weeks prior to vaccination and, as we know, it takes about two weeks before the vaccines have much impact. This means that deaths soon after a first dose, or after a later dose where the effectiveness of the previous dose has waned significantly, aren’t impacted by vaccination. Consequently, we are able to compare deaths soon after vaccination with deaths at a later date, once the vaccination has worked its ‘magic’, to see the impact of the last vaccine dose. We should expect deaths to decrease rapidly as we get further away from the date of vaccination.
As I was interested in the deaths of younger people I focused my analysis on the 40-49 year-old cohort. Fig 1 shows the number of deaths of 40-49 year-olds recorded by ONS in the 15 months from January 1st 2021 to March 31st 2022 by week following vaccination. The ONS report covers about 530,000 deaths in England (from all causes) across all age cohorts, of which 3,640 were deaths of people in the 40-49 age cohort.
In the chart below, the red line shows 3,514 deaths not associated with Covid, whereas the blue bars are the 126 deaths that were associated with Covid, week by week over the first 11 weeks post vaccination. I included the non-Covid deaths to highlight the issue of the healthy-vaccinee: people close to death may not be vaccinated, which is why the week immediately following vaccination has an artificially low number of deaths. It’s perhaps just worth noting that Covid deaths in this age group represented just 3.5% of the total, meaning if you’re in your 40s you’re 28 times more likely to die of something other than Covid.
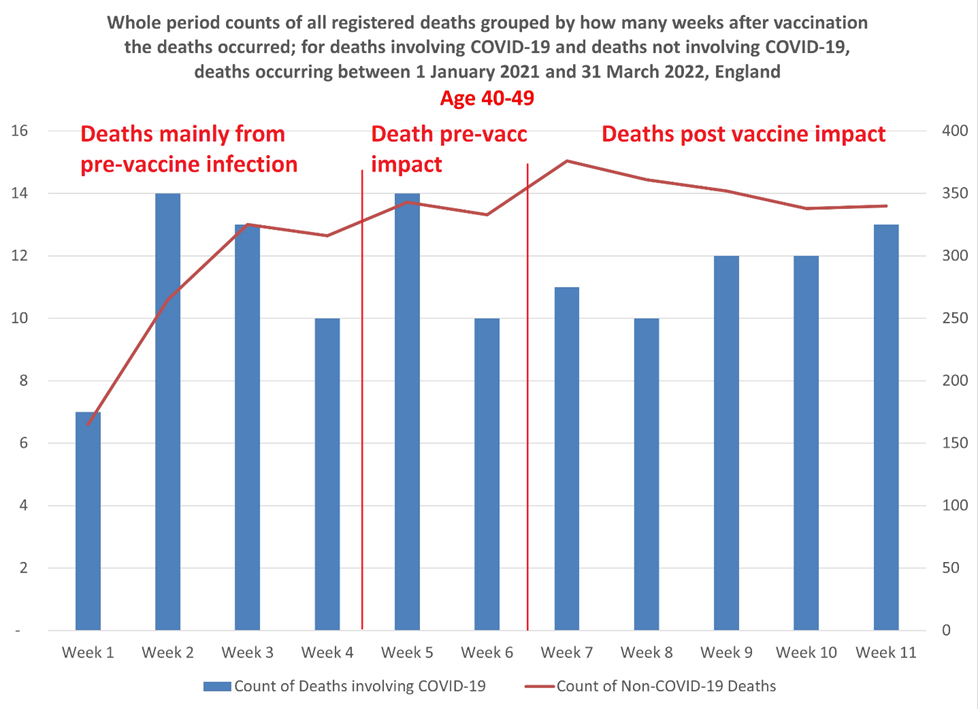
Just to clarify, deaths occurring within one week of vaccination are put into the “week 1” group. Deaths occurring in the second week following vaccination are allocated to “week 2”, and so on up to week 11. Deaths occurring 12 or more weeks after a vaccination are grouped into a single 12+ group. For the purposes of this analysis I’ve only looked at deaths in the first 11 weeks.
In the chart I’ve separated the weeks into three groups:
- Deaths mainly from pre-vaccine infection, these are the deaths occurring in weeks 1-4 following vaccination. Average deaths per week were 11.
- Deaths pre-vaccination impact. These are those deaths occurring in weeks 5 and 6, where it’s likely that infection occurred around the time of vaccination but before the latest vaccination would have had any impact. Average deaths per week were 12.
- Deaths post vaccine impact. Deaths occurring in weeks 7-11 are likely to have been of people whose vaccination should have reached full effectiveness by the time they were infected. Average deaths per week were 11.6.
Remarkably, the average number of weekly deaths in the first six weeks after vaccination was 11 whereas deaths during the period from week 7 to 11 averaged 11.6. Deaths actually increased in the later five weeks compared to the first six weeks.
The average number of weekly deaths in the last three weeks (week 9-11) was 12.3, as high as any other consecutive three week period during the 11 weeks.
This doesn’t look like 90% efficacy against death to me. Of course, many of these vaccinations are a second or third dose of vaccine, so perhaps we shouldn’t expect such a dramatic reduction in deaths, assuming the earlier doses are already giving some protection. But surely, if the efficacy has declined sufficiently to justify giving an additional dose, we should be seeing some impact of the latest dose?
But let’s just check the lag times involved. Naturally we’d expect relatively low deaths in the first few weeks after vaccination because people presenting for vaccination were supposed to have been clear of the virus for four weeks. The surprise here is that any one at all died of or with Covid in weeks 1 or 2; yet deaths in week 2 were the joint highest with week 5.
The ONS has estimates of the most likely time lags between infection, hospitalisation and death as follows:
- The time between COVID-19 infection and symptom onset varies between one and 14 days, with an average of five to six days.
- The median delay (lag) between symptom onset and hospital admission varies between one and 6.7 days depending on age and whether the patient lives in a nursing home.
- Time between symptom onset and death from COVID-19 ranges from two to eight weeks, with reported median times of 16 or 19 days.
This suggests a median time from infection to death to be about 24 days, with the shortest period being about 17 days. Yet in week 2, deaths are as high as in any week. Wouldn’t this indicate, as Fenton et al. suggest, that many of the deaths are simply miscategorised?
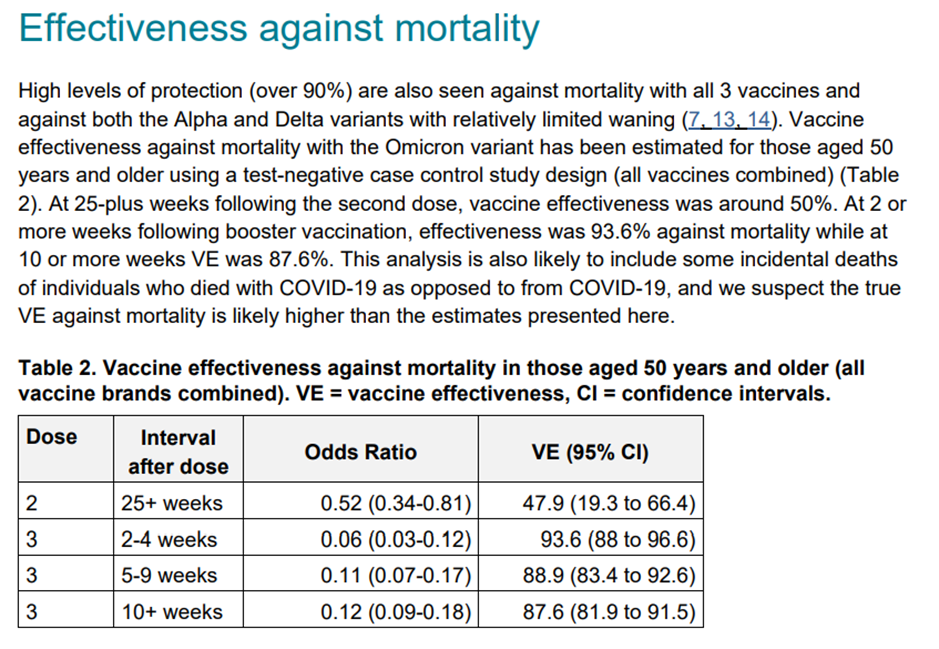
The official narrative would lead us to believe that fatality rates during weeks 3, 4 and 5 would increase to the prevailing rate of non-, or not-recently- vaccinated people as these are people who were clear of virus prior to vaccination and whose vaccine impact shouldn’t kick in a week or so after vaccination. The UKHSA weekly COVID-19 vaccine surveillance report (see below) claims 93.6% efficacy against death after two to four weeks for the over-50 cohort; I don’t suppose its claim for efficacy in 40-49 year-olds would be very different. This means that we should expect to see fatalities dropping off dramatically after about week 5. But we don’t; in fact, deaths start rising again after the middle weeks.
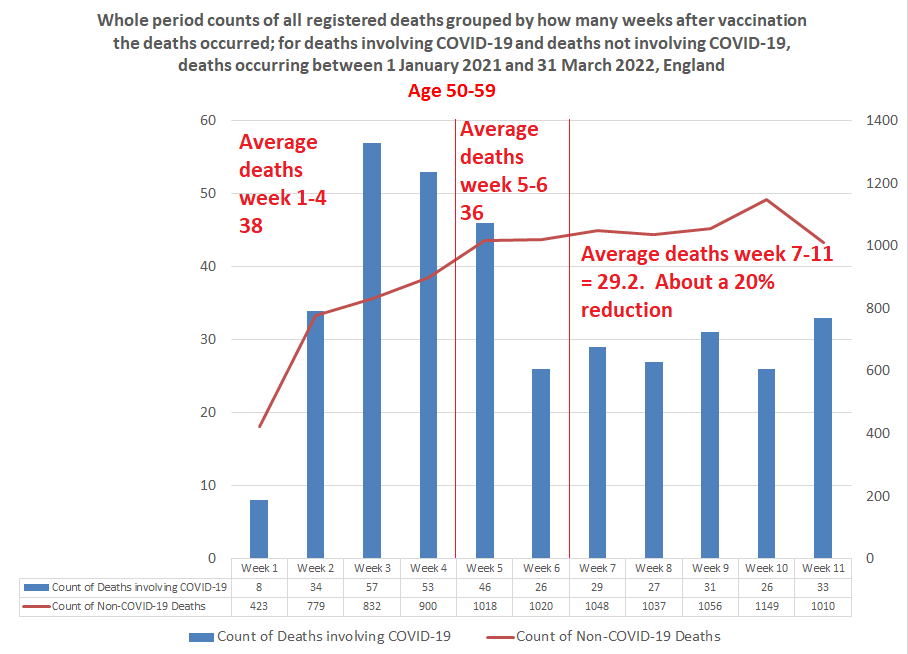
The picture for the 50-59 year-old (see below)) cohort follows more closely the profile of deaths following vaccination that we’re led to expect. Deaths in the first week or so after vaccination are low, rising in week 2 and 3 before declining. However, deaths in the last five weeks are only about 20% lower than the average number of deaths in the early weeks, though about 40% below the peak weeks. Still, this is a long way from the reduction in deaths we might expect given 90%-plus efficacy. What’s more, from week 7 deaths appear to be rising modestly. Has the vaccine effect already worn off?
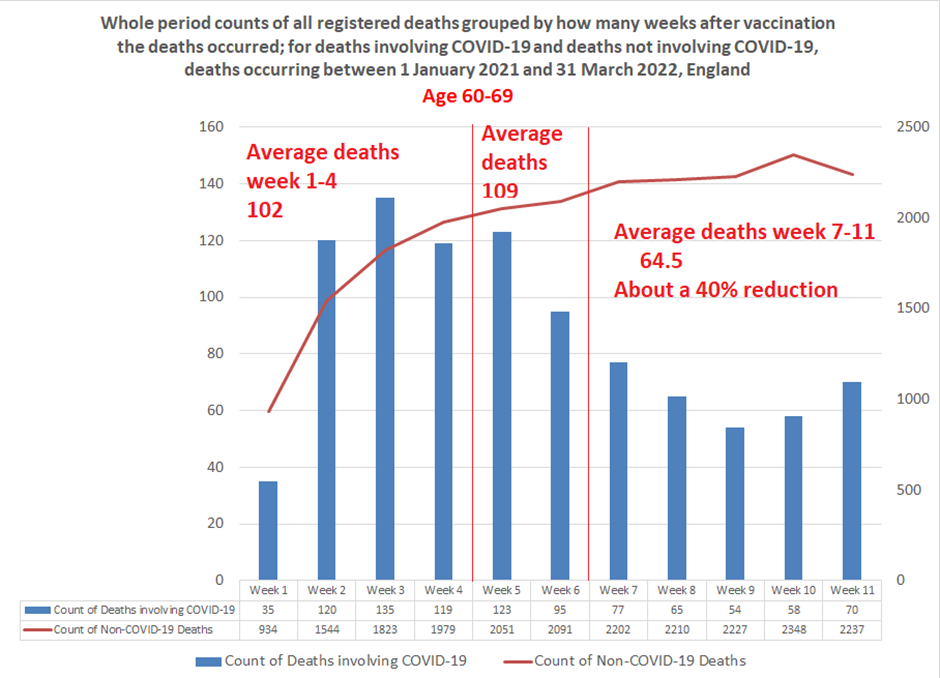
Deaths amongst the 60-69 year-olds (see below) again seem to follow the predicted path. However, the trough in week 9 at 54 deaths, a drop of 60% on the week 3 peak, appears short lived. Indeed, by week 11 deaths have climbed back up by 30% to 70. Overall, deaths in the final five weeks at 40% or so below the earlier weeks still seems a long way short of the claimed level of efficacy against death.
We keep hearing that vaccine efficacy is short lived. From this real-world data it appears it may be absent altogether in the 40-49 year-old cohort and both shallower and transient in the 50-69 year-old cohorts – though we must allow that efficacy from previous doses may be confounding the estimates.
What to make of it? I’m not sure. For me, the fundamental problem is that I’ve lost confidence in the data released by the various Government bodies and even more so in their interpretation of that data. Time and again we see that real-world data doesn’t match the narrative and rather than explain the discrepancy the real world data is simply withdrawn. Personally, I’m as sceptical of the claims that vaccines are doing untold harm as I am that they’re doing untold good. By continually overstating their benefits and understating their risks there’s been a huge growth in vaccine resistance. About 25% of the people who had their first dose haven’t had a booster, with this drop-off most marked in the younger age groups. With real-world efficacy data like these, we should hardly be surprised.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“What to make of it? I’m not sure. For me, the fundamental problem is that I’ve lost confidence in the data released by the various Government bodies and even more so in their interpretation of that data.” Exactly where I’m at. We’re reliant on data produced by people who have a vested interest in what that data supposedly proves. Much of the data is open to interpretation because of confounders like behaviour, definition of ‘covid death’ etc. so it’s impossible to draw a clear, definitive picture of what’s really going on. However, there is a general trend in acknowledgement of ‘vaccine’ efficacy issues and of ‘vaccine’ harm, and that trend is an upward one. I see it like this: if the government had to change the source of their data in the reports (shifting to triple vaxed, because the double vaxed was looking terrible), then pull the data altogether, then they know there’s a problem with what the data shows. But even without data, we all have a huge amount of anecdotal evidence that the stuff doesn’t work very well (or at all). My wife works at a GP surgery and almost everyone phoning up with Covid is triple jabbed.… Read more »
I’m glad I declined the offer back in March 21, as it’s panning out.
The problem we vax’d face is that rather worrying double-jabbed data back in December. The data that showed that we’d almost been turned into junkies. The data was that the double-jabbed had higher death rates than the unvaccinated and we had to take the booster to get the death rate to about the same as the unvaccinated. However, as we all know, that effectiveness is very short lived.
My brother who has underlying health problems has just messaged me to say he’s been offered the spring booster. I’ve said I’m not having it because of all of the above but he is more vulnerable (heart not directly respiratory).
This is a horrible position to be put in. In more normal times, I’d certainly say “seek medical help” but you just can’t get chats with your GP these days on subjects like that.
..sorry Rob, I feel desperately sorry because I know it’s really hard…
my friend is immunocompromised and in the same position..what do I say? The truth is I don’t think she should have any more, but I’m neither medically qualified or willing to say that. It has to be a decision for each individual.
I personally believe what Chris Whitty said, right back at the beginning…because it was when they were actually telling the truth…and it’s what I’ve seen with my own eyes…that for the vast majority.. it’s nothing more than a bad cold..whether you are fit, imunocompromised…or anything else…
Unless you are very old and at deaths door already there’s not a great deal to worry about, in my (non-medical) opinion.
I am absolutely livid that people have been put in this position by the lies and disinformation from both Government and the medical professionals..all backed up by the egregious MSM….I will never forget or forgive them.
“I am absolutely livid that people have been put in this position by the lies and disinformation from both Government and the medical professionals..all backed up by the egregious MSM….I will never forget or forgive them.”
Hear hear!!! They have a lot to answer for hyping everyone up, no questions asked (apart from of course “why didn’t we lockdown earlier?” Argh!). How they sleep at night I really don’t know.
Great article, thanks for carrying out the analysis.
I have been thinking and it is really unlikely that as a standard person you would notice in your life if the jabs were causing harm. Anything but death and really serious injury is just put down as from getting covid or side effect of jab that is worth it for the protection of gives. Only awareness of death would make a standard person stop and think(maybe!). So if 1 in 1000 did die from the jab as a standard person with less than 1,000 daily contacts, it remains hidden. It is only if the MSM get hold of this narrative that a standard person gets to become aware of it.
It looks like we are on the back foot in getting the message out!
The fact they have stopped producing the data – and many countries never published proper data to begin with, even though they must have it – says all you need to know. If the vaxx worked, there would have been no noticeable wave in autumn 2021/winter 2022. There would be no summer wave that is now higher than those of summer 2021 and 2020. If the vaxx worked, no or virtually no vaxxed persons would be infected or developing symptoms, certainly they would not be ending up in hospital or dying. The unvaxxed should be the only ones getting infected and falling ill and if that were the case, you may rest absolutely assured that they would be shouting that from the roof tops. When Pfauci said last year, around May 2021, that the vaxxed didn’t need to test, that said it all. Easy to say the vaxxed were not getting infected if they weren’t testing in the first place. No test, no infection – some ‘science’ that. Except reality showed up that lie very, very quickly – Israel was starting on it’s 3rd vaxx by July 2021. I find the bit about VE in age cohorts 50 and under… Read more »
Yes, a terrible waste of resources, and the attention to covid at the expense of every other illness known to man is criminal. Unfortunately I can’t see this changing any time soon. It seems to me many people are actually proud of getting Covid, as if it’s some sort of badge of honour, which, of course, is why a certain type of person will never give up testing themselves.
And have we really got a ‘wave’ of covid at the moment? I am so jaundiced by the behaviour of the msm, I tend not to believe anything I am told anymore. I can only say I know no one with covid atm. (Mind you, I have NEVER known anyone in my family or friends who has had covid – it it always a ‘someone’s aunties brother’ type thing.)
…I agree I’m sure that Prof Fenton, and Claire Craig to name two, pointed out that even when the UKHSA were publishing data most of the VE was assumed by modelling, and we all know how that works now!
Like many people I don’t know one person who died from actual Covid and nothing else, and if the FOI’s I’ve seen are true, it’s not surprising, as I think only a very few thousand have.
I couldn’t agree more that people don’t actually want to see with their own eyes..the ONLY people getting repeated bouts of Covid, are the jabbed. If it works, as you say, why have all the fully jabbed countries now got worse covid death rates than before…?
you don’t really need to be a statistician….and we still have no idea on long medium or long term side effects…..
Lies, damned lies, and statistics.
We are drowning in a sea of contradictory data.
Logically protection against death must be reduced somewhat for the current vaccines, that were formulated against a virus that went extinct 18 months ago.
I fear for my friend who had 5 doses, as he’s ‘immunocompromised’.
…well he probably is now, if he wasn’t before…my lovely friend has been talked into having three of the damned things at the same time as under-going cancer treatment…..she’s only in her 40’s and is just getting over Shingles…Surprise!!
One of the most diabolical things about this whole charade is that in the original trials there were NO immunocompromised people (similarly there were No pregnant women)…not a one….so anyone saying they needed it more was basing it on what??
And as no one seems to factor in deaths and injuries from the vaxx in their supposed efficacy studies (in fact they seem to completely ignore that they are happening)..
I fail to see how they can ever produce anything that shows true ‘effectiveness’…if a major piece of evidence isn’t even being addressed!
‘This makes it effectively impossible to see if claims for vaccine efficacy turn out to be substantiated.’
Which is exactly why they stopped releasing data.
But anyway it’s a meaningless exercise.
The virus is ONLY likely to cause serious disease and death within less than 0.5% of the population under specific conditions, age around life expectancy AND with comorbidity, or younger but in poor health, so using data from the rest of the population to ‘prove’… what? That vaccination prevented people from hospitalisation or death who anyway would not have been hospitalised or dead?