Evidence of Increased Infection Risk Following Third Dose, Exacerbated by Vaccination Drive During Omicron Wave, UKHSA Data Show
Despite all the mess that are the official sources of data regarding Covid infections, hospitalisations and deaths, we should at least be grateful – not only that they give us a chance to glimpse beyond the spin-doctors and into the reality of what’s going on with the pandemic in the U.K., but also that the data are also giving us insights into the way diseases propagate through the population.
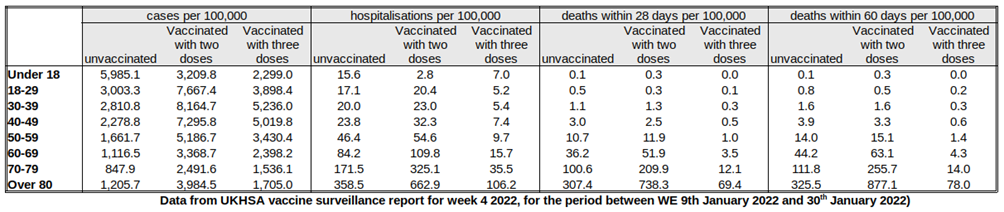
First of all, just to make things clear – Table 12 in the UKHSA Vaccine Surveillance Report once again shows data for those triple-jabbed rather than two-or-more doses, as was given for the data for 2021 since September. However, we can estimate the rates for those with only two jabs using data in Tables 9-11 and vaccination data available from the NHS. Using these data we can estimate infection rates by vaccination status (above); from these data we can then estimate the unadjusted vaccine effectiveness for infection for those having two or three doses (below). The infection rates continue to be considerably worse in the vaccinated, both double and triple jabbed, translating to highly negative unadjusted vaccine effectiveness estimates. Note that these figures are rates per 100,000 so take into account the different sizes of the cohorts, meaning it’s not because there are more vaccinated people than unvaccinated.
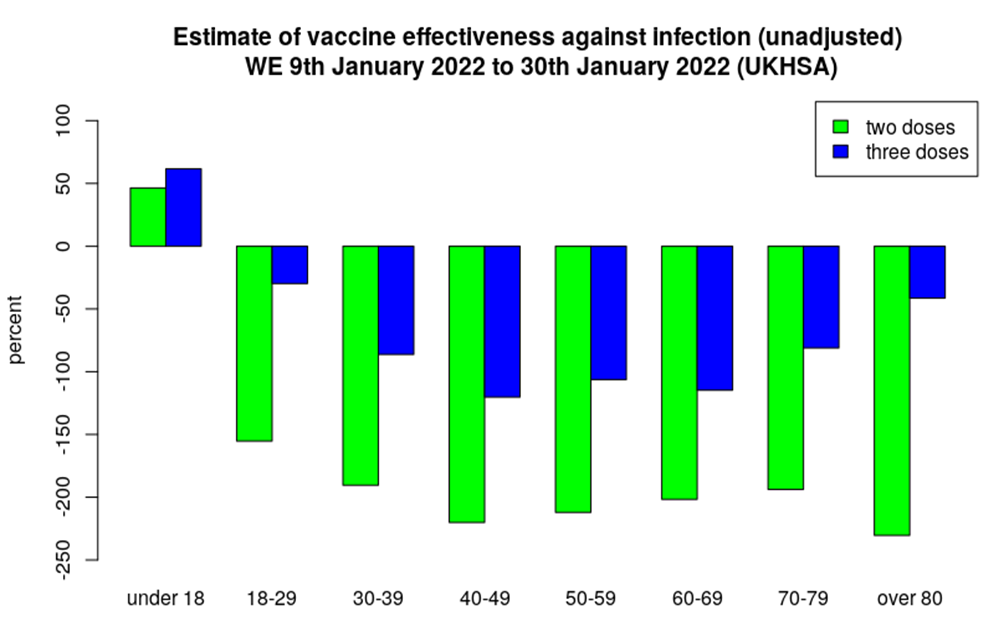
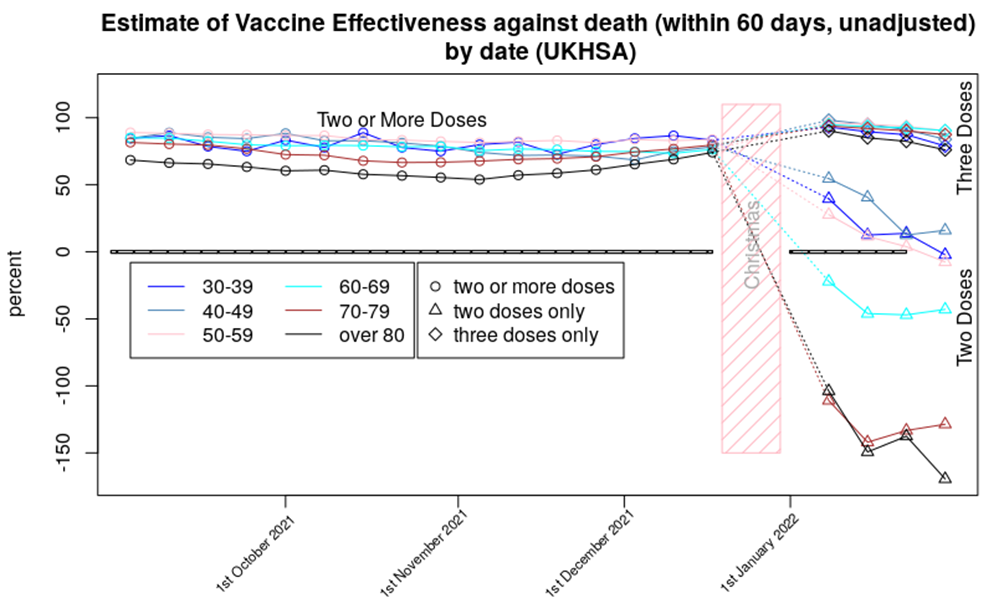
It won’t immediately be obvious from the above charts, but what we see this week is the infection rate in the triple-vaccinated continuing to worsen, but an improvement in the infection rate for the double-vaccinated. This then is reflected in the estimated vaccine effectiveness – better for two doses, worse for three doses. This can better be seen in the graph of the change in unadjusted vaccine effectiveness by age and dose, below. Note the scale on the y-axis, and the fact that all values are negative, most considerably so, reflecting higher infection rates in the vaccinated, both double and triple jabbed.
In that chart the rebound in the vaccine effectiveness for those having had two doses of vaccine looks rather remarkable.
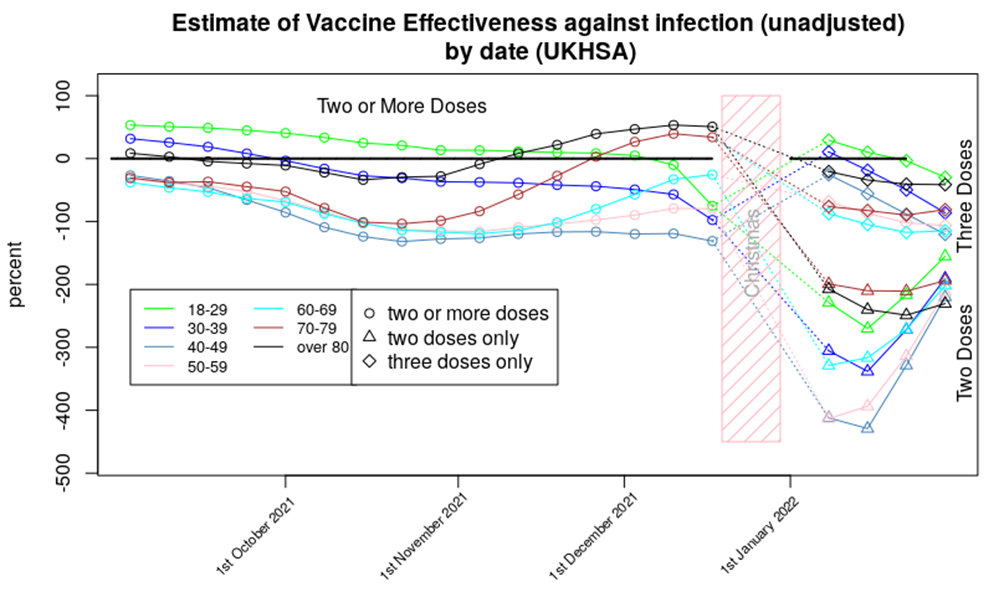
Of course, this is difficult to explain as a simple ‘change in vaccine effectiveness’ – we all know by now that vaccines wane in their effectiveness, but while it is possible for vaccine effectiveness to get better, this is always seen close to the point of vaccination as the immune system response to the vaccine matures. We don’t tend to see such significant improvements some time after vaccination.
So what’s going on? While there are several potential mechanisms to explain this sudden drop and then recovery, I believe that the most likely explanation is that we’ve fallen foul of some of the the small print in the data: “Third dose 14 days or more before specimen date.” More specifically, we have already seen that there is an increased risk of infection in the three weeks following both the first and second doses of vaccine; it is likely that a similar effect is occurring after the third dose. The “14 days or more” in the small print means that if there were increased infection rates in the recently boosted then these cases would be counted within the data for the double-dosed.
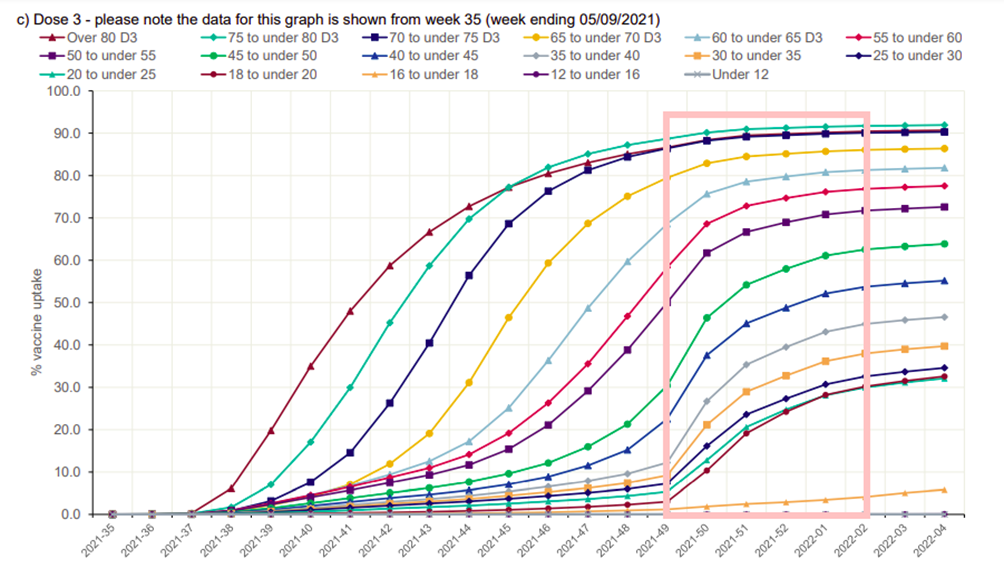
Is this effect enough to explain the sudden increase in cases in the double dosed? Looking at the booster dose rollout data (below), it is clear that the time window for the low point in the vaccine effectiveness curve for the double-dosed is aligned with the rollout of the booster programme in those aged under 40, and there were still high booster-vaccination rates for those aged under 70 around weeks 48-49. Note that the data for the week two and three 2022 vaccine surveillance reports actually come from weeks 49 2021 to week two 2022, which I’ve highlighted in the pink rectangle.
A reasonable question to ask at this point is why this effect wasn’t seen before. I suggest that it is likely that this effect was responsible for the dip in vaccine effectiveness seen for older age groups from October 2021, just before the impact of the boosters resulted in vaccine effectiveness increasing once more from November. It is unfortunate that we don’t have data for two and three doses separately for this time period, as these data could have supported the hypothesis that the drop in vaccine effectiveness was an effect due to the ‘recently boosted’ having higher infection rates.
There remains the question as to why the dip in vaccine effectiveness was so deep during the first few weeks of this year; this is almost certainly due to this being the peak of the Omicron wave. I have heard many times that it is foolhardy to undertake mass vaccination programmes during an epidemic wave, and these data likely show why. Note that it isn’t just that the recently boosted would have been more likely to be infected – they’d also be likely to infect others, making the peak of the epidemic wave higher than it would have otherwise been. This effect is true of negative vaccine effectiveness in general – the current data suggest that the impact of the vaccines, including those boosted at the start of the booster programme, will be to have more cases than we’d have had if we had only vaccinated the most vulnerable, with concomitant increases in hospitalisations and deaths.
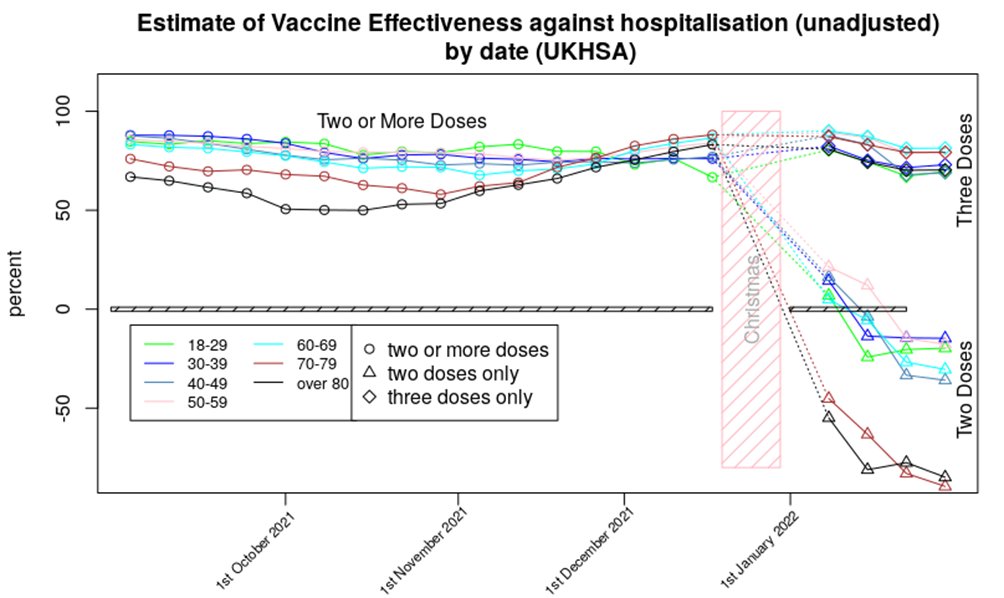
The hospitalisation data show only minor changes from last week’s report. The vaccine effectiveness against hospitalisation for those aged 70 and over shows a continued fall; the double-vaccinated in this age group now appear to be approximately 75% more likely to be hospitalised compared with if they’d never been vaccinated. It is possible that this is due to a ‘healthy vaccinee’ effect – I discuss this below. While it is possible that we’re seeing a delayed version of the ’14 days or more’ effect mentioned earlier, note that the most negative vaccine effectiveness is seen in those aged over 70, who had their booster doses some time ago; I don’t think this effect explains the increased risk of death that we’re seeing in the data.
All that said, I’d suggest that those aged over 70 are very likely to be vulnerable to Covid and thus would benefit from a booster. This would likely offer them protection against hospitalisation, with short and medium term side effect risks likely to be lower than the health risks they face every day (which are substantially greater than found in the healthy young). While questions remain about longer term impacts of the vaccines, in the short term at least they seem to be offering some protection to the elderly and infirm. With this in mind the important aspect of the very negative vaccine effectiveness seen in the chart above is what it tells us of the risks that might come for the non-vulnerable vaccinated. Also, it is important to remember that the elderly are used to having to take medicines to counteract the negative consequences of other medicines, or continuing to have to take medicines to stop the negative consequences of withdrawal – this is not a situation that the healthy young are familiar with, and in my opinion there would have to be significant benefits of a medicine or treatment to make exposure to this type of ‘lifelong medication’ worthwhile.
The gap in unadjusted vaccine effectiveness between those aged under 70 and those aged over 70 appears to have increased slightly. It is possible that this reflects the time delay between the first vaccinations for the vulnerable in January 2022 and the rollout of the vaccine into less vulnerable groups a few months later. Alternatively, this gap might reflect age-related changes in the immune system and how it responds to the vaccines.
The data for vaccine protection against death shows a mildly worsening picture compared with last week’s Vaccine Surveillance Report, with negative vaccine effectiveness for two doses of vaccine seen for all age groups over 30 other than the 40-50 age range where there is still some positive effect of vaccine. Of course, the series of well-defined data points suggest precision, but in reality there will be uncertainty around each data point – without additional data it is difficult to add error bars or confidence limits. I’d suggest that it is best to consider that two doses of vaccine offer around zero protection against death for those aged under 60. The situation for two dose vaccinees older than 60 is more complex – the data strongly suggest that these individuals will have an increased risk of death compared with the unvaccinated, but I again note the possibility of a ‘healthy vaccinee’ effect, that is, where the increased death rate in the double-vaccinated actually reflects those most close to death not being given a booster. Without data on the morbidities of those that die (and that are hospitalised) it is impossible to confirm or deny the presence of this effect.
That said, last week I considered that if were are seeing a ‘healthy vaccinee’ effect then we should expect to see those very negative effectiveness figures for protection against death from two doses of vaccine for those aged over 60 rebound a little further and then flatten out over the next few months. I don’t think we’re seeing this effect yet.
Note that I present the data for deaths 60 days from a positive test, rather than the normal 28. This is because the data suggest that the vaccinated have a relatively high risk of death in the 28-60 day period, compared with the unvaccinated; this suggests that the vaccinated have a slower disease progression, but with similar outcomes. I would very much like more data on this potentially important subject, but more data isn’t available (a common problem with any data that might show the vaccines in a negative light – compare this with the extraordinary efforts being taken to identify more cases of the mysterious Long Covid).
Finally, one point not shown in the data above: U.K. reported cases have flatlined since mid-January at around 90,000 cases per day, and mortality is still hovering at its recent peak of approximately 250 deaths per day. But perhaps this is to be expected – in the U.K. we get around 50,000 to 120,000 cases per day of OC43, the most common variety of ‘coronavirus cold’, and perhaps an average of 50-100 deaths a day within 28 days of catching an ‘OC43 type cold’, with more during winter and fewer during summer. Is our current situation not far from where we’d expect to be once Covid became endemic in this country?
In summary, the latest data suggest that:
- Infection rates continue to be elevated in the vaccinated, with even those boosted seeing higher case rates than the unvaccinated.
- The increased risk of hospitalisation for those with only two vaccine doses appears to be getting slightly worse
- The increased risk of death in the double-vaccinated compared with the unvaccinated continues to be troubling.
- It is likely that our current infection rates are getting closer to what would be expected from an endemic ‘common cold’ caused by a coronavirus strain. Hospitalisation and death rates appear to remain slightly high on that comparison.
Amanuensis is an ex-academic and senior Government scientist. Find him on his Substack page, Bartram’s Folly.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Jolly good, just as I always thought; contracting flu naturally and recovering naturally really does work. Especially if you keep yourself fit, eat well, sleep well, spend less than you earn, avoid debt and invest the rest.
The flu vaccine is one of the most widely used vaccines in the world, our government bride our corrupt GPs to shove it into as many older people as they can.
The fact that it doesn’t do any good at all is considered irrelevant.
Anals of Internal Medicine
The Effect of Influenza Vaccination for the Elderly on Hospitalization and Mortalityhttps://www.acpjournals.org/doi/full/10.7326/M19-3075
‘The data included 170 million episodes of care and 7.6 million deaths. Turning 65 was associated with a statistically and clinically significant increase in rate of seasonal influenza vaccination. However, no evidence indicated that vaccination reduced hospitalizations or mortality among elderly persons. The estimates were precise enough to rule out results from many previous studies.’
Pharma and the GPs get a fat pay day out of it and I’m sure the political vermin get their cut as well.
The interesting thing about this is the potential for influenza being primarily spread by superspreaders, and not using the familiar ‘measles’ model where each infected person spreads it to a few others.
The potential exists for the flu vaccine to increase the chances of a given person becoming a superspreader.
Thus you could get protection at an individual level, which is what is measured in the clinical trials, but at population level you’ll get more superspreaders and thus more infections in total — this increase in infections would tend to ‘cancel out’ the benefits of vaccination.
The highly important aspect of this is that so long as you only vaccinate the most vulnerable you have a chance of erring on the side of net vaccine benefit. As you vaccinate more in the non-vulnerable group you’ll push the equation towards negative protection at population level. (ie, because the young don’t get seriously ill from influenza, but can contribute to spread if they’re more likely to become a superspreader).
“Anals of Internal Medicine”. Quite a Freudian slip there!
Politicians have to get rich somehow, poor things.
God, that is FAR too sensible – but my life and professional experience tells me you are 100% …….right.
And the “Thoughts” of your “namesake” reside by my bed for occasional inspiration; I recommend them to all.
“All that said, I’d suggest that those aged over 70 are very likely to be vulnerable to Covid and thus would benefit from a booster. This would likely offer them protection against hospitalisation, with short and medium term side effect risks likely to be lower than the health risks they face every day”
be amazing to see the positive effect Ivermectin had instead of a booster, n’est pas Amanuensis?
Yes. The evidence for ivermectin grows stronger with every study. It also appears to be holding onto its effectiveness with newer variants.
Really we should be trialling the vaccine against ‘easy’ treatments.
I’d still imagine that there’s a place for vaccination, but only in those most very vulnerable to covid (which, if you remember, was the original stated intention of the vaccination programme).
My wife and I (54, 50, both unvaccinated) had Covid and recovered in two days. We took ivermectin and other bits and pieces; my highly sceptical wife was converted immediately when her symptoms eased dramatically within an hour of the first dose. Could be psychosomatic, could be coincidental, it’s certainly only anecdotal, but that’s our little story.
How did you get hold of it? I would like to have it on standby but don’t know how to get a reliable source
I can’t say how I got it but I believe there are people who have ordered it from overseas, or bought it overseas and brought it back.
Obviously you are taking a chance on reliability, especially with the former.
I and many others from the boards at Going-Postal.com have used a company called Guru Baba Pharmax in India. Feel free to ask over on Going Postal for confirmation.
We contacted a source in India but they replied asking for a prescription.
I was back to 100% strength after 6 days and only felt rough for 2 days. I went down the easier route of Vitamin D3, Vitamin C and Zinc. They have made it so hard to get hold of Ivermectin, it’s pretty criminal that some people resort to the horse paste variety, but apparently the product quality is high for animals.
There are ways. But I hope and pray that Matt Hancock grips the rail over this.
I’d prefer it if he walked the plank.
I think he should be given all the vaxxes daily and film of it being administered broadcast to the nation.
And let’s not forget Quercetin either. And Niacin too.
Robert K Jnr demonstrates with devastating effect by referencing trial and field data that IVM – and other early treatment anti virals – could have rendered this virus scam null and void; that is not being wise after the event by him and the medics and scientists he cites because this was mooted from very early on; we now know how the nexus of Fauci/Gates/Zuckerberg/Big Pharma/criminally acquiescent Governments and their health quangos such as MHRA/ UK CMOs and CSOs/ compliant MSM organs have all combined to thwart the use of these drugs by medics. The result is: deaths and induced ill health of millions of entirely innocent and unsuspecting people; enrichment of big Pharma, already rich Tech oligarchs, compromised Government quangos such as NIH/NIAIH by holding revenue producing patents and shares in Pharma companies thus making their actions to promote these jabs wholly criminal. It may not have been a concerted conspiracy as some have suggested, but it certainly appears to be a bandwagon jumped on swiftly and with full vigour by all this truly evil cohort. If this is not pan continental genocide as some have suggested – I would love to hear how the ProJab apparatchiks who frequent… Read more »
What an unmitigated disaster the vaccine programme has been. And we are only just seeing the beginning of that. Hubris is a bitch.
Read the vaccine surveillance report.
Sorry but it ain’t a vaccine -it’s genetic therapy
Yes and they even told us so!
Not even that, it’s a genetic modifier.
It isn’t a vaccine, but I insist on calling it one. It was only called a vaccine so that people who questioned it could be labelled “anti-vax”.
However, the fact it is failing so badly – and that people are increasingly waking up to that fact – gives us an opportunity to de-weaponise the term “anti-vax”. Anti-vax works as a term because the general public view vaccines as infallible medical miracles that only a fool would refuse. When they realise that there can be good and bad vaccines, just like any other fallible field of medicine, then questioning a “vaccine” loses its stigma.
So yes, absolutely- the failing, dangerous and unethical programme we’ve been subjected to is definitely, 100% a failed vaccine programme.
‘Take this unlicensed drug now. It’ll make you much more likely to contract this disease, but slightly less likely to die of the disease you’re much more likely to contract.’
I don’t remember Sir Lenny Henry saying this on TV, do you?
‘Get vaccinated. You’ll be up to three times more likely to be infected and you’ll be helping to protect you and your loved ones from absolutely nothing at all.’
David Walliams
A well know medic?
Why would he need to be a medic? The ability to read would be sufficient.
Well known medics like Harold Shipman and Josef Mengele? You’d sooner trust them than David Walliams?
A well known moron
A well-known glove-puppet, with a BBC hand up him, nodding to the narrative.
‘Getting vaccinated against Covid-19 is the most senseless decision you’ll ever make. It will help to keep you and those around you infected with Covid-19 constantly and protect you against serious illness for a small and ever-diminishing window of time on an endless regimen of state sponsored coercion.’
Jim Broadbent
A well know medic?
Why is this relevant? Explain, please.
I think we’ve picked up another dose of the 77s….to go with the (ir) rational one.
It could be the same person or a variant.
Or even a Scariant.
The zero brain cell variant cf the one brain cell variant
Better to use the term ‘vaccinologist’ or similar — medics are highly trained at treating people for disease, not drug development.
A well known moron
That’s twice you’ve posted that question. If you’re likely to do it again, could you at least type ‘well-known’?
I remember Jim Broadbent being all for it In the Beginning. I recall him on some sort of celebrity presentation. Am I remembering incorrectly?
No….. only perhaps Sir Chris Whitty
Take the “vaccine” but please make sure you die within 14 days of taking it so we can chalk you up as an unvaccinated death stat.
Do any actual drowning casualties get recorded as drowning or are they still get logged as Covid deaths?
“And it’ll be your fault it doesn’t work if you won’t take it.”
More on nanotech in vaxxes.
I do not think we ought to be scared off from discussing these topics by fear of ridicule, the reports keep coming in, and some are well based.
https://robinwestenra.blogspot.com/2022/01/new-zealand-scientists-have-found.html
Ridicule is well deserved.
What do you mean by nanotech?
What do you mean by ‘mean by’?
Another subject being ignored by the so-called sceptics, not palatable to their narrative.
I recomend you view Dr Kevin McCairns PhD microscopic investigation of the vaccines (many examples on McCairndojo.com) he found a lot of contamination (except in sputnik), but the “nanotech” claimed by others was not evident, he did find a lot of crystalisation (saline solution was used as a control, exactly the same phenomina was observed) similar to what others claimed to be nanotech. Bubbles were also observed, these have been erroneously claimed to be magnetic spheres by others. McCairns live microscopy also observed vaccine blood interactions, compulsive viewing for anyone considering the jabs IMO, hemoglobin was rapidly stipped from bloodcells, cells swelled, the edges where the vax met the blood on the slide showed considerable clotting. There does seem to be a circle jerk of patrion farmers making these nanotech claims, La Quinta columbia lost all credibility after their first Spanish study showed an example TEM pic from the literature, although the lab could not find any GO using TEM, all subsiquent english translations claimed GO was found, using the example picture as if it was produced by the lab. This is evidenced in the Whitney Webb GO video on TLAV. Others making the same nanotech and other “tentacled creatures”… Read more »
Some of these claims sound as incredible as the government’s advice that everyone should get covid vaxxed, but rather less well-funded as propaganda goes.
If you source Dr Richard Fleming, he has also highlighted not only the effect of these jabs directly injected in to the blood stream, but also the detritus he found in a sample batch of all jabs ….
Are these interpretations based on “Unadjusted” data, with uneven sizes of cohort.
Unadjusted in terms of the morbidity etc of the individuals, but they are adjusted for cohort size and age.
I’d very much like it if the government sponsored a few large matched cohort studies which would get around the problem you state — but they’re not doing this, and prefer to spend all their cash on marketing to get people to become vaccinated and the ineffective ‘track and trace’ programme.
As it stands these are all the data we’re getting. As it exists at population level it should even out the characteristics in each group and shouldn’t be too far off, but yes — proper data would be very useful to have.
Short summary:
The vaccines program has been an unmitigated disaster.
It has sucked up all the money and resources from all other areas of healthcare; the Government are spending the same amount on debt interest as we do on defence (not that we protect our borders but we will protect Ukraines); if you are struggling with energy bills we’ve got some nice tax increases for you; we need more money to protect the NHS but it won’t protect you.
wrong.
Hello leek. I made 7 statements in my post – if you’d like to let me know which ones you disagree with and perhaps your reasons why I’d be happy to consider if you are correct in labeling any of them as “wrong”.
Paying money on debt interest is a political choice. There is no need to pay any interest to anybody at all. We can stop doing it tomorrow.
Yesterday the Chancellor handed £2.25bn to banks over the next year and nobody batted an eyelid. Quite how paying banks more money is going to reduce the amount of money demanding goods and services is one of those unanswered mysteries of life. Largely because the answer is: it doesn’t.
If you don’t like it, then lobby to have KPI1.1 at the Debt Management Office suspended and all Gilt auctions stopped. Then you’ll see who the free money from the state has been propping up.
No need to worry: an “independent” Judge has decided the National Fund cannot be used for charitable purposes so its c.GBP650 billions are held for the Nation – and are, presumably held “off balance sheet”.
So , Rishi, and BoE, borrow and QE away for a bit longer……I reckon you have c. GBP250 billions of headroom before “there is no money left” …
The amount of people I know who have come down with COVID shortly after getting “the jab” suggests to me that it really does make you more susceptible, at least in the short term. A couple of my friends have blamed this on the long queues they endured to get “their booster.” I just nod and smile. They may be right but it never seems to occur to them that maybe, just maybe, these “vaccines” are not as effective as advertised.
Little steps… but slowly getting there!
Must have been all those dirty unvaccinated waiting in line for their booster.
Pretty much every study has identified this effect for jabs #1 and #2. There’s a presumption that it is occurring for jab #3. This is exactly why the data always starts at >21 or >14 days post vaccination.
The problem (from an epidemiological point of view) is that they mix the <14 days since booster (in this case) data in with the data for the double jabbed — they should be presented separately.
Pretty much everyone I know who has been vaccinated has got it. It has put a lot of them off their boosters, amusingly.
If you’d been vaxxed, you wouldn’t want that to be true, either.
https://jermwarfare.com/blog/reiner-fuellmich-covid-exit-strategy
Reiner Fuellmich on Jerm Warfare discussing covid exit strategy.
Reiner Fuellmich : the bravest and most outstanding defender of Humanity and champion of the exposure of Covid Evil Lies and Falsehood on the planet!
If we survive this genocidal bio-warfare against all humanity, he will be the ultimate hero.
Effectiveness against symptomatic disease Vaccine effectiveness against symptomatic COVID-19 has been assessed in England based on community testing data linked to vaccination data from the National Immunisation Management System (NIMS), cohort studies such as the COVID Infection Survey and GP electronic health record data. After 2 doses of the AstraZeneca vaccine, vaccine effectiveness against the Omicron variant starts at 45 to 50% then drops to almost no effect from 20 weeks after the second dose. With 2 doses of Pfizer or Moderna effectiveness dropped from around 65 to 70% down to around 10% by 25 weeks after the second dose. Two to four weeks after a booster dose of either the Pfizer or Moderna vaccine, effectiveness ranges from around 60 to 75%, dropping to 25 to 40% from 15+ weeks after the booster. Vaccine effectiveness estimates for the booster dose are very similar, irrespective of the primary course received (3). Vaccine effectiveness is generally slightly higher in younger compared to older age groups. Effectiveness against hospitalisation Several studies have estimated vaccine effectiveness against hospitalisation in older ages, all of which indicate higher levels of protection against hospitalisation with all vaccines against the Alpha and Delta variants (6, 7, 8, 9).… Read more »
They compare their vaccine effectiveness to those that have not had the illness naturally and recovered.
A fairer comparison would be between naturally recovered and those artificially exposed by way of injection.
The naturally exposed and recovered are much better protected from future illness because natural immunity is much longer lasting across numerous variants whereas the injections required regular boosters.
Relative or absolute? The difference is fundamental to understanding.
It would be helpful if the authorities spent more time explaining to the population who are at risk from covid. They’ve done the opposite and scared everyone.
If the population don’t know this it is because they have been living under a rock. It has been explained repeatedly.
The behaviour of the public suggests that most people massively overestimate their risk from covid, except for the most vulnerable who seem to underestimate it slightly.
This effect has also been seen in surveys.
I’ve not seen any official sources explain the low risk from covid in the non-vulnerable. I have seen plenty of official statements that say that everyone is at risk, with the implication being ‘similar risk’.
I’ve always been a sceptic on this matter, and have taken a greater interest in it that almost anyone of my acquaintance. So, I’m fairly confident that if the government had been telling me repeatedly about relative risk from covid among the various cohorts within ‘the public’, I’d have noticed.
efficacy of a treatment is always expressed as relative. Otherwise you are not assessing the treatment.
Had you read and understood the surveillance report, it would be obvious to you.
You would then have understanding.
Leek, cutting and pasting from CVSR without wondering whether ‘they would say that, wouldn’t they?’ doesn’t do you much credit and exposes you to a charge of weak critical thinking.
As a product of UKHSA, CVSR is not an independent piece of work and it presents much of the data in such a way as to mislead or obscure. After all the lies and propaganda of the last two years, you cannot criticise people for questioning it.
Even the text you have quoted is so scientifically imprecise (“was associated with a vaccine effectiveness of…”etc) as to be virtually meaningless, even if it wasn’t already contradicted by much of the statistical data elsewhere in the report.
Hello Private Leek – backing up your troop movements along with Pt Rational I see.
How are you getting along with boot camp? Hard to learn cut and pasting eh?
Never mind, you’ll be back in your comfy Mum’s basement when your shift is over.
They use test-negative case-control. If you look at some review papers for the method (just do an internet search — I won’t pre-select one for you) they pretty much all state that this method shouldn’t be used for vaccines with the characteristics of the covid vaccines.
Please ignore this idiot.
So 8 people disapprove of this good news. Why?
Go to c19study.com and read up on the success – real world – that medics the world over have achieved by treating patients EARLY rather than waiting for viral loads to be higher and only putting people in hospital when they have got …sicker.
And you should read how these medics have found IVM and HCQ to be very effective at defeating the virus in double quick time – especially those in Utter Pradesh.
Early treatment anti viral repurposed drugs (with no statistically relevant record of death and adverse effects) effectiveness versus death and adverse effect inducing “vaccine” effectiveness…….. which would you rather have?
As others have stated, the difficulty for you is trusting the Pharmas to do a Cochrane standard assessment of their drugs – they do not have the best track record with that or did you not know that – as well as determining the difference between “RRR” and “ARR”…
Regarding “vaccine” effectiveness against hospitalisation and death.
The vaccinated have been told that it stops them needing hospital treatment which creates the placebo effect whereby a vaccinated person who catches Covid doesn’t feel the need to go to hospital because they’ve been told by a “higher authority” that they are protected. This skews the figures in favour of “Vaccine Effectiveness”.
Conversely an unvaccinated person with exactly the same symptoms have been told via propaganda they are likely to die and will therefore present themselves to hospital through fear which again skews the figures against the unvaccinated.
All these “healthy vaccinee”, “unhealthy unvaccinated” and vaccine induced Covid patients within 14 days of the jab (regarded as unvaccinated in some studies) are skewing the figures making the jabs look a lot more effective than they really are (if they are effective at all).
We all know that the ONS has grossly underestimated the unjabbed population by the many articles on this website.
I still believe the jabs are totally unnecessary and cause a lot more harm than good.
The value of vaccination, of 2 dose and of boosters slides with age rather quickly, since the risk for those healthy and under 40 is so low from Covid. The marginal benefit of vaccination at all doesn’t seem likely to be increased sufficiently by a 3rd dose to warrant cost and NHS resources dedicated to it. The concern is how much marginal benefit 3rd dose and potentially a 4th doses provides those 65+ and the immuno compromised. Because if it falls significantly and may cause immune system degeneration in any way, then we should stop at 3. A more towards curatives or a vaccine that targets the whole virus seems the better place for investment.
We all know the flu vaccine has a sometime woeful impact due to strain evolution. But because we have lots of curatives, we can handle that reality. Whatever the Covid version of Tamiflu eventually is decided to be (out of many competitors), that will be what protects us longterm. Not repeated jabbing, and especially not the lower age cohorts.
Perhaps you haven’t heard but Tamiflu never worked, it was always a pharma con.
In addition it isn’t that the flu vaccine is sometimes woeful, it is always woeful. It does not provide any benefit yet it is one of the most damaging vaccines going, perhaps it is because they still stuff mercury in it?
Anals of Internal MedicineThe Effect of Influenza Vaccination for the Elderly on Hospitalization and Mortalityhttps://www.acpjournals.org/doi/full/10.7326/M19-3075
‘The data included 170 million episodes of care and 7.6 million deaths. Turning 65 was associated with a statistically and clinically significant increase in rate of seasonal influenza vaccination. However, no evidence indicated that vaccination reduced hospitalizations or mortality among elderly persons. The estimates were precise enough to rule out results from many previous studies.’
Also studies have found that countries with higher flu vax percentages in the elderly also have higher percentages of “covid related deaths”.
This may be due to the vaccines harming the immune system leaving it more open to respiratory infections and or that they preserve the very elderly thus leaving more low hanging fruit.
Sorry unable to provide link but believe it was in a Cochrane report about 18 months ago.
The other issue with the ‘flu jabs is that from early last year, the NHS widened the age range to encourage it’s use. It’s now age 51 or more. I’ve no idea whether it’s been taken up as intended, but as it only has a short ‘shelf life’ during any year, it’s entirely possible that they have to scrap a lot of it each year.
I don’t disagree with what you say but I feel where the medical profession have fallen down is to go along with the idea that you can outsource personal responsibility for your own health to big pharma. If you look at the NHS deaths in hospital since March 2020 96% of all fatalities had a ‘pre-condition’. The predictor of a good/bad outcome from a dose of covid, or flu is general health not how many vaccines you’ve had.
Clearly, there are unfortunate people who have debilitating conditions but I continue to be amazed at how so many people allow themselves to become so unhealthy.
It takes effort to stay healthy.
As people age they think of their health the way it was 20 years before — you’ll find people in their 50’s talking of running fast or playing football like a pro — but it is fond recollection, not their current state.
When reality comes calling and they realise they’re obese etc, it is very difficult to claw yourself back into health.
I agree. One of the most illuminating studies during the whole farargo was a Zoe one fitness after lockdown 1. It boiled down to the people who were fit before the lockdown got fitter, the unfit for unfitter! About 3kgs gained v 3kgs lost a delta of 6kgs & a few points on the BMI scale.
BTW, excellent graphics, I like how you’ve shown the divergence of 3x vaxxed from prior 2x.
Yep
I’d suggest that anyone who feels comfortable with the drivers behind Big Pharma should watch the TV series ‘Dopesick’, which deals with the actions of the drug company (and the FDA’s complicity) during the Oxycontin opioid scandal, which addicted large swathes of the US while being touted as ‘1% addictive’.
We need some clinical trials to investigate this.
Instead they’re just going ahead full steam.
https://stevekirsch.substack.com/p/my-statement-at-the-feb-4-acip-meeting
I have just 3 minutes. I’ll be talking about 3 reasons that they should not approve the Moderna COVID vaccine. I’m confident they will ignore everything I say; they don’t want to hear it.None of the ACIP committee members will talk to me. They ignore everything I send, including my offer to donate $1M to a charity of their choice if they would just answer my questions on a recorded zoom call.
They are not interested in seeing the safety signals we found either. The FDA and CDC don’t want to see those signals either. I’ve tried numerous times and gave up.
https://rwmalonemd.substack.com/p/the-us-public-health-response-has
Malone’s latest substack.
Some very brave whistleblowers are exposing the new leaked data out of the DoD on what is happening to our servicemen. The death and disease statistics for 2021 are shocking. Later today or tomorrow will be the big release of the validated data discussed at the Senator Ron Johnson hearings last week.
I will get the data up as soon as I am able tomorrow on as many channels as I am able. Please share when I do – let’s make this viral! Stay tuned!
Everyone has a choice in this battle, this battle for good and evil. For our children’s well being. For our soldier’s well being. For our populace’s freedom. Censorship, propaganda can only last if we all let it.
Malone: Covid Hero – one of about a dozen of the most outstanding
A friend of a friend is a super bedwetter and has been since day one. However, his wife keeps on testing positive which they think is due to the fact she know keeps on getting nose bleeds from shoving a stick up her nose and blood getting into the test solution. Apparently they are going to test less now.
Should I spread it around that super bedwetter lives with somebody who’s positive and should permanently quarantine?
Send them details about Chinese anal swabs.
It will open up a whole new world for them.
China Using Anal Swabs for COVID Testinghttps://www.webmd.com/lung/news/20210128/china-using-anal-swabs-for-covid-testing
Apparently most Tories were doing these years before covid came along, all the rage at no.10 parties.
The rate of reinfection is troubling.
It would be very useful to see some data on reinfection rates in vaccinated vs unvaccinated.
So the cure spreads the infection – sounds like Mafia plot!
Oh….wait!
Any sheep still asleep?
Oh dear ……only millions.
I was speculating the other day that the whole partygate thing has been set up and implemented by Boris to distract from the abject failure of the vaccine programme.
Throughout the national disaster that has been the lockdown policy the one thing the Tories have puffed their chest up about are the vaccines and the speed of the roll out.
If it is widely acknowledged that the vaccines actually make things worse then Boris and the Tories really are up poo creek.
Having Boris publicly criticised for allowing parties is a minor issue in comparison, a nice distraction for a far bigger failure.
But every time a politician talks about easing of restrictions, it’s always thanks ‘to our amazing vaccine rollout.’ What utter shite.
Yes indeed. They gave pharma a massive blank cheque and pharma served up mass murder in return.
After extensive research it seems my preferred course of action and relying on my own natural immunity, following infection in late 2019, seems to have been vindicated and been proved correct.
Not trying to be a clever dick, I just have faith in my own health and body.
My grandmother always said you should rest, if you got a cold, “to give your body chance to fight it”.
When you felt a bit better, you should go for a walk in the fresh air, to “loosen the cold, then you can blow it away”.
Never failed. She supplemented it with whisky with hot water and sugar before bed on the worst days. She lived to be 90. And was barely troubled by colds or flu.
Feed a cold, starve a fever
Sounds like my grandmother! A very wise lady – she did have a whisky and water every day though, not just when ill!
I’d very much suggest vitamin D supplements as well — everyone in Europe is vitamin D deficient during the winter months and into early spring, and the impact of vitamin D on regulation of immunity is well known.
Work colleague yesterday reported that yet another of her friends / acquaintances has “gone down with covid”, which she claims is “rife” where she lives.
I asked if they were ill, or what symptoms they have. Oh, no symptoms and most are not ill, but they have tested positive and are isolating “to be on the safe side”. I pointed out that if they weren’t at all unwell, they most probably had a dodgy test result (or were skiving, though I didn’t add that bit.)
And yes, they are all vaxxed. I didn’t find out why they were testing themselves, but from what bits I hear of her group, they are all covifanatics, so probably do it as a matter of course. Vaxxes working well then.
You can’t help some people!
So if you are 70 and only have two jabs should you have the booster? On the face, the data support it. BUT if two jabs render one so vulnerable with time, will the booster render you even worse over time. Secondly, the first two jabs were AZ but the booster would be Mrna. Thirdly, might the vaccine effect wear off in time to a point where it is effectively the same as unvaxxed? Fourth, Omicron is less severe than delta and past experience implies future variations would be less serious. My father and his parents lived well into their 90s, so 20 plus years for the unknown longer term effects of Mrna vaccines to manifest. A conundrum.
Yes, i am getting a bit fed up of hearing that over 70s are ‘vulnerable’ and should have the vaccine and boosters. I read early on in this s***show that a healthy and fit 70yo can have a much better immune system than an overweight and unfit 40yo so I really don’t think these wild generalisations are any help.
I am 71, fit and healthy, take my vit D every day. I have never had a flu or heaven forbid covid jab and seldom get anything other than the occasional cold and since starting the vit D hardly any of them. i did have something back in autumn of 2019 remarkably like covid though, not very serious although the cough lasted a long time.
The idea that the elderly don’t have much to lose from any long-term effects of the jabs is as you say a bit cock-eyed, many healthy 70yos could well live for another 20 years, plenty of time for these effects to show up.
The ageing of the immune system is complex. We really need much more research of the impact of overall health on covid risk.
If you’re taking vitamin D supplements make sure it is over about 1,200 IU a day during winter/spring. Below this level the benefits are marginal.
Rather sadly, the point about ‘risks’ is real. It isn’t about how long it takes for risks to turn up, but what risks are taken day by day anyway. If a treatment increases annual risk of death by 1% (in absolute terms) then you might not even see the impact in the mortality rates for those aged over 80, but for those aged under 30 it would be a massive increase in mortality.
I am 70. I know someone of 83 who had covid but it was no worse than a cold. My BMI is just over 23.My blood pressure and pulse are the same as an average man in his early twenties. I exercise regularly and can easily walk12 miles without thinking about it . I am lucky with my genes but have looked after myself. I take a high safe dose of vitamin d3 and vitamin c in the winter with occasional zinc. I had the two AZs because we were told it would help stop the spread.. Ha! I have decided not to have the booster for the time being and regret having had the two AZs. My choice. If I’m wrong, my fault.
I’m still in two minds whether there will be a net long term benefit of vaccination for the most vulnerable.
I’d suggest that there is probably a point where ‘it is worth it’, but that age/morbidity is difficult to ascertain.
No conundrum. Don’t go near the injections.
Been a while since the drug treatment has been in the news actually hasn’t it? Are they getting spooked.
“All that said, I’d suggest that those aged over 70 are very likely to be vulnerable to Covid and thus would benefit from a booster. This would likely offer them protection against hospitalisation, with short and medium term side effect risks likely to be lower than the health risks they face every day”
If we deny them their boosters, will we be able to Look Them In Their Eyes?
Get your boosters, you old folk, or you’ll get Covid and end up in hospital!
On the other hand, we could reduce their heating bills, and make sure they can afford to eat properly.
From December 2020:
£252m to Ayanda Capital, registered in Mauritius for tax purposes. PPE not delivered
£186m to Uniserve. PPE not delivered
£116m to P14 Medical Supplies, with assets of just £145. PPE not delivered
£108m to PestFix, with just 16 employees. PPE not delivered
£107m to Clandeboye Agencies, a sweet wholesaler. Yes, a sweet wholesaler. PPE not delivered.
£40m to Medicine Box Ltd, with assets of just £6000. PPE not delivered.
£48m to Initia Ventures Ltd, which registered itself as “dormant” in March. PPE not delivered.
£28m to Monarch Acoustics, which makes shop furniture. PPE not delivered
£25m to Luxe Lifestyle, which has no employees, no assets, and no turnover. PPE not delivered
£18m to Aventis Solutions, which has total assets of £332. Not a typo, £332. PPE not delivered
£10m to Medco Solutions, incorporated just 3 days after lockdown, with share capital of (not a typo) £2. PPE not delivered
In all, approx £1bn to inexplicable suppliers for PPE that hasn’t been delivered.
incredible
Where did you dig those up from Foxy?
I think Mark Steyn over at GB News would like to get his hands on those data
I saw something similar on the Good Law site, Jo Maugham.
We’ve had their new definition of vaccine, it only seems right and proper that we should return the ball with a new definition for Government Spending Policy:- Event Horizon.
There is so much fraud to investigate, yet I imagine very little will be and the establishments courts will let the prosecuted few off with light sentences. The system looks after it’s own and their families.
Hell’s Bells.
Israel going through a remarkable surge in cases and deaths
https://ourworldindata.org/covid-cases
https://ourworldindata.org/covid-deaths
Israel has exceeded its peak death rate for the entire pandemic this last week
everyone has about 4 jabs, including 5 year olds and the Omicron variant is no worse than a runny nose
how does that work?
They redefined vaccine herd-immunity & pandemic…
This jus “redefines” protection to mean vulnerability.
Huge jump in COVID patients in ICU too. So the vaccine clearly isn’t preventing serious illness there.
The data coming from Israel is remarkable.
It should be headline news.
Also, watch to see what happens in New Zealand over the next 30 days.
I do hope it’s not bad news for that nice Miss Ardern.
Do you think it is Original Antigenic Sin amanuensis?
The Silent Olympics: Beijing Restricts Free Speech
https://www.theepochtimes.com/the-silent-olympics-beijing-restricts-free-speech_4254927.html?utm_source=uschinanoe&utm_campaign=uschina-2022-02-04&utm_medium=email&est=969zSkyV1JMnbz4N2yVxKKgjVKRSmwZkXB6LuAuachB7EOVsJRVf5xyo%2F5fSB%2BdKGW%2Fw
By Antonio Graceffo
Saturday 5th February 2pm
Windsor Great Dog Walk for Freedom
behind one simple sign
“Covid Rules Are Barking”
All Canines and Humans welcome
Even if you don’t own a dog please come along
meet Alexander Park (near Bandstand) Barry Rd/Goswell Rd
Windsor SL4 1QY
Stand in the Park Sundays 10am make friends, ignore the madness & keep sane
Wokingham Howard Palmer Gardens Cockpit Path car park Sturges Rd RG40 2HD
Henley Mills Meadows (at the bandstand) Henley-on-Thames RG9 1DS
Telegram Group
http://t.me/astandintheparkbracknell
According to the royal-decorated Wellcome Trust director Jeremy Farrar, using the Torygraph’s “science correspondent” Joe Pinkstone as his foghorn, anyone who says SARSCoV2 may have come from a laboratory is putting “the world at risk of a new pandemic”.
In short, being sane in public is anti-social – and far, far worse than going nuts with a submachine gun at a school or a railway station.
Imagine even talking about SARSCoV2 when you suffer from lifelong mental rabies.
Keep on going Joe, and maybe they’ll make you a “Sir” one day, eh, you creep?
Excellent article as always. It is a rare talent to be able to make such complexity understandable, for a numpty like me.
No it is just anti-vaxx nonsense. Targeted at people who don’t understand.
Then feel free to put your challenge forward and enlighten us all.
Just saw some charts and believed them…..
Read the original report. You will see..
Children’s mental health: Huge rise in severe cases, BBC analysis reveals
https://www.bbc.co.uk/news/education-60197150
well done BBC – this is your lockdown – you wanted it so badly
How is this related to vaccination effectiveness?
I’d like to complain about the poor quality of trolls on this site!
Can’t they send someone at least partially competent to lie to us?
Perhaps we are viewed as the front line, the dirty trenches where 77 send their latest recruits to bloody them.
If they survive the battering here perhaps they are let loose on such as The Daily Fail.
Drinks all round.😀
The cabal that runs the media keeps up the lies and hatred against the un-jabbed. A very small group of corporations and individuals own virtually all the media world wide. Isn’t it about time we asked why Great Resetters such as the Murdoch family are still obsessed with jabbing everyone on the planet? Also Mr CNN Ted Turner (the man who allegedly funded the Georgia Guide Stones) has the same obsession.
Doesn’t anyone in the general public think it is a bit odd? and resembling CCP style societal control more every day. Can barely think of a single person working in MSN who shouldn’t lose their jobs for inciting genocide.
Dear Amanuensis
Can you show your calculations, where you derive negative effectiveness against hospitalisation or death.
The unadjusted data rates in table 13 of the vaccine surveillance report does not support your conclusions.
You can email them at lockdownsceptics@gmail.com
I’d like to see the justification on here. Obviously the claims are not justifiable from the data. It’s just a pack of lies.
My point was that they may not read the comments – but I could be wrong
I don’t think you understand the data. It’s very clear.