Latest Covid Hospital Data: Community Admissions Falling in London, Tailing Off Nationally
We’re publishing the latest update from our in-house doctor, who’s pored over the latest NHS England and ICNARC data packets so you don’t have to. Contrary to some hysterical reports in the media yesterday, it’s actually good news. Community admissions for Covid are falling in London and tailing off across England – and of those classified as being in hospital ‘due to Covid’, 40% were admitted for something else and only have Covid incidentally.
When I was a medical student, a novel called The House of God was required reading. It relates the experience of the fictional American Dr. Roy Basch in his first year as a qualified doctor. The book contained lots of good advice for surviving the junior doctor ordeal including several ‘Rules of the House’. Rule 13 states: “The delivery of good medical care is to do as much nothing as possible.”
Surprisingly often in medicine, doing nothing is the best option. One of my former mentors frequently advised me to “do as little as possible for as long as possible” – his point being that over-hasty intervention is not just unnecessary, but can be actively damaging. This transgresses a key principle of medicine Primum, non nocere – first, do no harm.
Having looked at lots of data from multiple sources over the last few weeks, I am coming to the view that the entire country would be better off in almost every way if doctors stopped ‘doing things’ for a while – particularly if they stopped testing asymptomatic people for the variant du jour.
I will discuss the available information and explain why I have arrived at that conclusion.
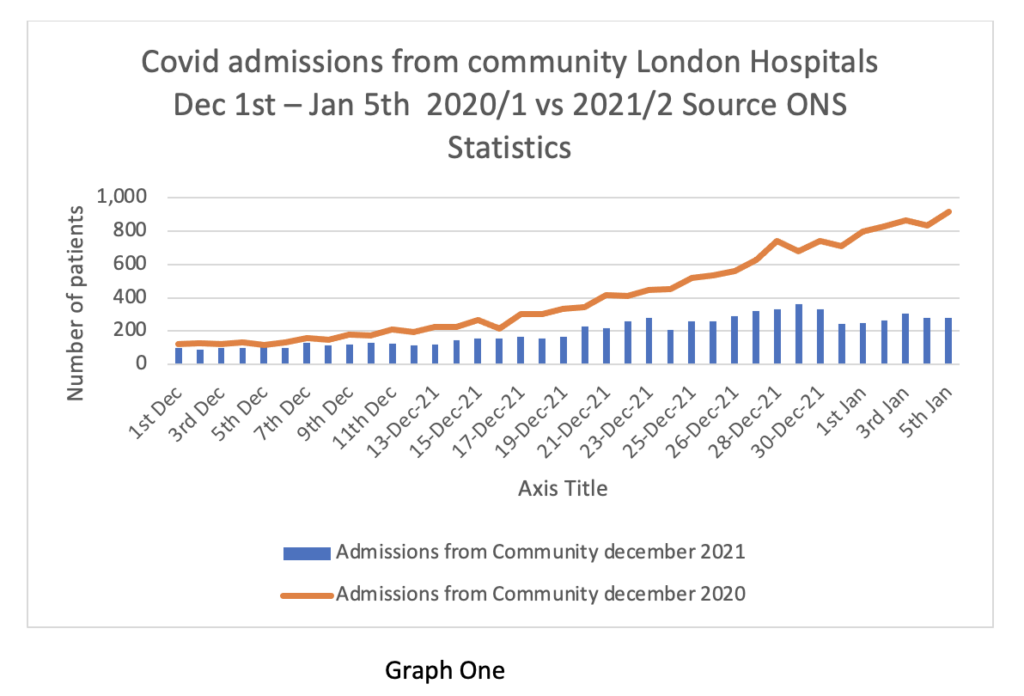
Firstly, the admissions from the community in London (as the leading edge of the Omicron wave).
Graph 1 shows the daily Covid admissions from the community in the blue bars vs the same time last year on the brown line. Readers will recall that Professor Sir Chris Whitty warned at the Downing St press conference on December 15th that a big increase in Covid hospital admissions after Christmas was “nailed on”.
It looks like we are waiting for Godot, because the numbers are actually falling, not rising and are currently less than a third of levels a year ago.
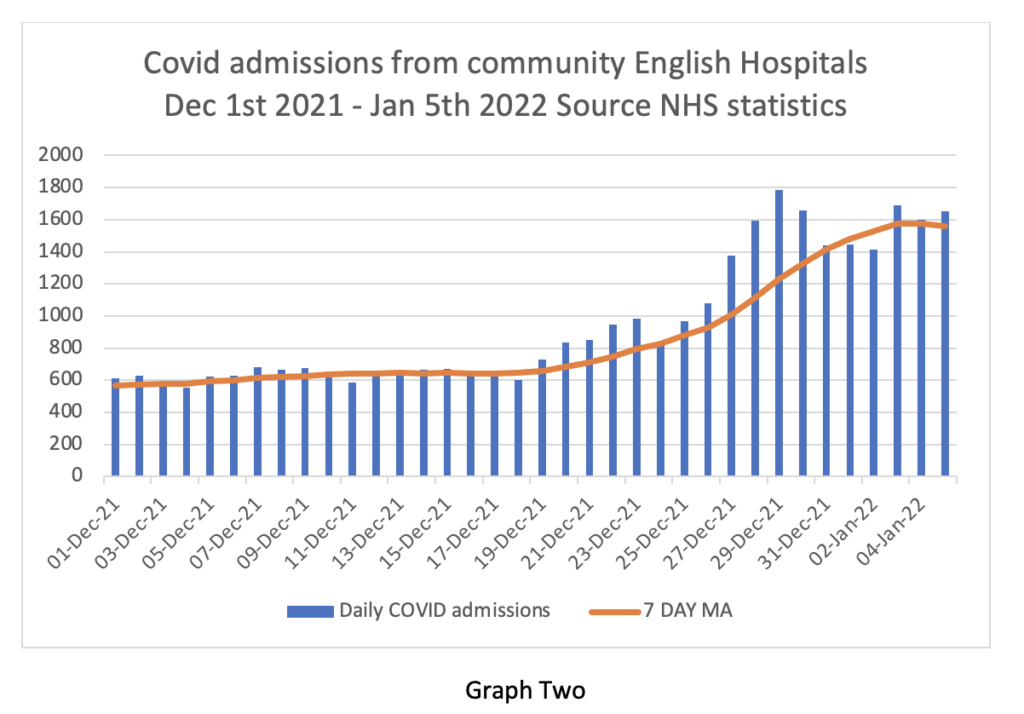
Graph Two shows the same metric for the whole of England. On this graph the bars represent daily admissions, the brown line the seven-day moving average. Again, admissions to hospital from the community are tailing off.
This is not really surprising as the ONS data for community infections shows that London appears to be well past the peak. The same pattern is also seen in the ZOE app reports. Other regions are now showing rising positive tests for Omicron – and it is likely that regional waves will peak and decline rapidly, as in the capital. Rather oddly, the data for Wales seem to show much higher community spread of Omicron than in England, despite far more stringent social restrictions. Could it be that Mark Drakeford’s draconian rules aren’t flattening the curve? Whatever next?
On Thursday/Friday the NHS release a weekly summary with hospital level data and the Primary Diagnosis spreadsheet. Graph Three shows the Primary diagnosis data for English hospitals – a busy graph, so I will explain it. The vertical bars represent patients testing positive for Covid (orange) and patients being ill from Covid in hospital (blue). The difference between the two is the number of patients with ‘incidental Covid’ – in other words, they’ve tested positive but that’s not the reason they’re in hospital.
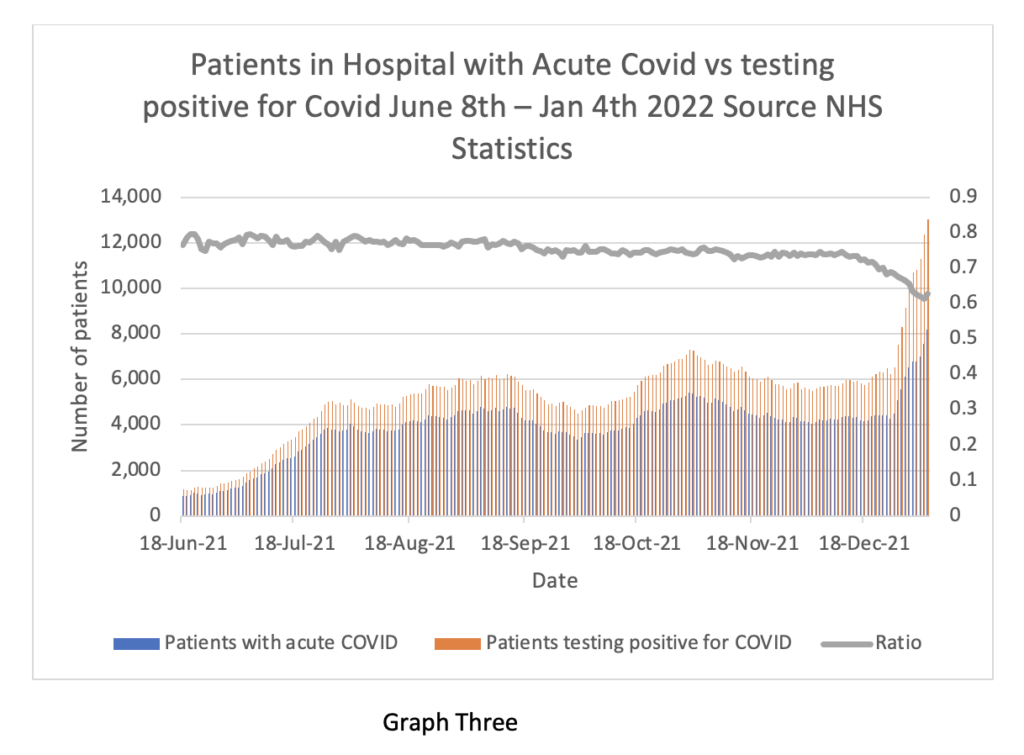
It can clearly be seen that the ratio between the two on the gray line is falling quickly – in other words, only 60% of the total patients reported as in hospital ‘due to Covid’ have actually been hospitalised because they’ve got Covid. Fully 40% of the patients in the reported totals have Covid as an incidental condition. In the Midlands, 45% of patients have ‘incidental Covid’. I expect the proportion of incidental findings will increase in coming weeks. I will return to this point later in support of my contention that we need to rapidly scale back testing.
The weekly hospital update is often quite dull. Not so this week. For a few weeks now it has been apparent that hospitals in the East and South East of London have had higher admission numbers from the community than other parts of the capital. These numbers are now plateauing. However, the total Covid inpatient burden is much more evenly spread across the London hospitals. I think this indicates a serious issue with in-hospital spread of the virus (not surprising), although the significance is much less than in prior waves, because Omicron really is less severe than previous variants.
Exactly how much less severe is not possible to say because the NHS will not release key pieces of information around length of stay and oxygen utilisation in hospitals. Patients who are not very ill with Omicron do not need supplemental oxygen – it would be easy to compare current oxygen utilisation rates with those from a year ago to assess relative severity of Omicron vs the Alpha variant.
Readers may wonder why the NHS send this information daily to NHS Trust CEO’s but conceal it from the public? Readers may speculate that the NHS choses only to release information supporting the catastrophe narrative and conceals data supporting the opposite view. Readers may very well think that. I could not possibly comment.
The Spectator calculates that average length of stay has fallen from 8 days to 5 days – anecdotally I hear it is closer to 3 days. Admissions to ICU are flat and not substantially above normal for January, as are death rates. Cases of influenza, respiratory syncytial virus and community acquired pneumonia are all substantially below expected levels for this time of year.
Unfortunately, the latest ICU ICNARC report does not provide information around how many people have been admitted to ICU with Omicron vs Delta. I expect this information will emerge in time. It is certainly already known. Although absence of evidence is not evidence of absence, it is a reasonable assumption that if most of the current ICU admissions were positive for Omicron, the BBC would be broadcasting that fact on an hourly basis. So far, that dog hasn’t barked – I am not expecting to hear it.
Given all the evidence that Omicron is a variant of the common cold and that admissions of moderately unwell people seem to have peaked already in London, why is the NHS under so much pressure?
There are three main reasons. The first is the policy of sending staff home for extended periods of time based on positive lateral flow tests irrespective of whether they have symptoms.
The second is the incredible degree of ‘organisational friction’ in segregating patients on Covid wards and the arcane rules around testing prior to surgery.
The third is the difficulty discharging patients from hospital – so called ‘bed blocking’.
The first two factors are attempts to limit the spread of Omicron. The available data shows the futility of that approach. Omicron is so transmissible, eventually everyone in the country will be exposed to it – yet only a tiny proportion of people will experience serious illness – very much like the common cold. If persistent testing of asymptomatic people stopped tomorrow, a substantial number of problems currently besetting the NHS would vanish overnight. To quote Rule 10 of The House of God: “If you don’t take a temperature, you can’t find a fever.”
I have come to the view that we are making mistakes in management of the pandemic that will damage the country for years to come. Much of these mistakes stem from testing asymptomatic people for a disease which is highly unlikely to do them any harm.
I close with a well-known limerick, which contains good advice for our times: “Dr Bell fell down a well, and broke his collar bone. Doctors should attend the sick, and leave the well alone.”
Primum, non nocere.
Stop Press: Saturday’s Daily case toll fell by 20% week-on-week and Covid hospitalisations in London are 31% lower. MailOnline has more.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Never let the truth spoil the MSM propaganda.
The in-house doctor has pored over it, not poured over it, I hope.
If it had been little Macron.. he’d have pissed over it..
Yes …to upset the unvaxxed!
Napoleon would have ‘literally’ shat over it
Slightly worse than that.
The MSM of course mis-translated him. He actually said “smear with sh1t”
Not convinced that’s a limerick!
Just what i was thinking but a good little verse nonetheless!
Almost on topic when talking of limericks, illness, death and toxins:
There was a young lady from Ryde
Who ate some green apples and died
The apples fermented
Inside the lamented
And made cider insid’er inside
Johnson will blame the unvaccinated and call the graphs ‘mumbo jumbo’!
Dungford will then say that Johnson is following false Fascist mumbo jumbo, whereas the Dungs are correctly paralysing Wales by virtue of superior Stalinist mumbo jumbo.
Saint Sir Tony of Blair will call the doctor an idiot, and declare war.
He’s the geat jumbo lump, and I refer to the size of the empty chasm inside his head.
Many of the deaths in the first and second waves were caused by forced intubation of ICU patients NOT directly from Covid. Different treatment would have led to fewer deaths.
Omicron is no worse than a common cold, less people in ICU need ventilation and consequently the NHS is killing less people.
Time to get back to normal.
Why assume an ICU patient who has tested positive for omicron a) is actually infected with omicron and b) is NOT infected with delta or “original”?
I remain sceptical that omicron has caused even a single person to be seriously ill.
I was thinking that last night – how many people are seriously ill with Omicron? Especially if you remove the incidentals and the type of people that will be in ICU for any respiratory virus and I wonder if now the ‘medication’ is worse than the disease.
The PCR test is not able to distinguish between live or dead cells. A healthy person can test ‘positive’ from residual dead viral fragments of a long expired respiratory disease – but the ‘pandemic’ fraud requires every false positive to be deemed a covid infection. Taking that one step further, a person with a cold that develops into flu, who tested false positive, enters ICU as a covid patient. This is how they managed to make flu ‘disappear’.
Because Omicron is the dominant variant and there is far less Delta around and very little if any Alpha.
Excellent article in the Spectator today about the death of democracy includes the following:
‘we are basically now expending vast resources tracking the spread of a cold – and it is time for the Government to acknowledge this fact, lift all restrictions, end all emergency powers, and bring the state of emergency to an end’.
Watched the Chief Exec of Kings College hospitals on the British Biased Corp this morning, and he seems as empty headed as the rear of them, and gave the unveiled threat of mandatory vaccination in all but name for all staff.
There’s a fourth reason, possibly the most pertinent. Over the last 20 years, despite an increase in UK population of ~10million, the total NHS bed numbers have fallen by ~75,000
This is data that needs pushing constantly. Its something your average Joe can make sense of. Exactly the same has been happening in France.. in fact during the so called ‘covid crisis’ beds have been reduced by another 5000.
This bed reduction is cynical and premeditated, proving once again this covid nonsense is nothing to do with health..
Not forget that the Tories fired tend of thousands of care home staff because they weren’t stupid enough to take the gene therapy injections, this has screwed up the health care system even more.
“The delivery of good medical care is to do as much nothing as possible.”
Are you mad?
Where is the profit for pharma in that?
What you actually want is to inject perfectly healthy people, (who are an no risk of a disease) with a gene therapy drug disguised as a vaccine numerous times a year, now that is modern medicine, that is profit.
Of course the coup de grace being a vaccine passport so you can force people to take as many of your unecessary (and dangerous) injections as you desire, has their ever been more lucrative business?
I know I won’t get a reply to this post but I am curious about common colds so this is for thought only purposes. Catching a cold or flu virus, NHS advice appears to be, take a paracetamol, it should make you feel better and will keep your temperature down (interfere with my brains ability to control my body temperature). I see, so my brain is in fact superfluous. But surely raising my temperature is another defense mechanism and method of fighting a virus? Are you a doctor? No, just a someone who has been lucky enough to have a fully functional bullshit filter. You might also wish to take something for that blocked up nose, to make you feel better. I see, so my brain is again superfluous. But surely blocking up my nose is another defense mechanism, preventing me from picking up another virus and compounding my misery? Are you a doctor? No. As a thought experiment have you ever considered that a cold or flu virus could in fact be helpful? A way of keeping your immune system upto date and functional, perhaps during a cold/flu infection it could even be keeping rogue cells such as cancer… Read more »
I understood every word.. only doctors speak complete bollocks..
Spot on in all aspects.
Similar with aspirin. The wisdom is that it works by blocking the body producing, (amongst probably some other immune responses) prostaglandins which are there to protect and heal but which cause inflammation and pain.
So, aspirin reduces pain but delays the healing.
Simple trade off.
But, one for the real experts – precisely how does it achieve this?
Paracetamol doesn’t keep your temperature down. One of its side effects is to induce slight sweating, a natural way of slightly moderating an elevated temperature. Its main purpose is to alleviate pain.
A blocked nose and consequent coughing and sneezing is the means by which a virus transports itself. Your body isn’t protecting itself, it’s responding in the way the virus wants it to.
The rest I largely agree with.
On the subject of pain. I’ve noticed that with a good dose of flu my natural pain relief is reduced to the point where certain areas of my body, particularly those which have been previously injured, begin to hurt but I don’t take a paracetamol because I’ve noticed that when I start to recover, the natural targeted pain relief I receive feels better than before. More to consider perhaps.
I don’t want to question your medical knowledge but how often do you have flu? I haven’t had it for over 20 years, and before that I’m pushed to remember any other times except for when i had Asian flu as a child. Loads of people on this and other sites say they’ve never had flu and yet you talk about ‘a good dose of flu’ as if it’s quite a regular occurrence!
I would say I catch flu at least once a year, usually from close contact with one of my grand children, although nothing worthy of reporting since the end of 2019 or whenever everyone started wearing face masks, self isolating or keeping their distance.
I’m not a doctor, nor a medical practitioner, I have no special medical knowledge, just my observations from the 1950’s to date.
I would say you’re catching a cold at least once a year.
When you catch flu, it’s something you remember for the rest of your life – a real benchmark, which puts every other cold into perspective.
I have never sought a professional opinion from a doctor so it’s entirely possible. Can you define the symptoms and differences of a common cold and flu.
flu and the common cold is the difference between night and day. You will know if you ever get flu on account you can’t move for a good 5 days. Whereas you can function day to day with a cold.
I maintain it’s flu but it never wipes me out, I don’t remember any being noteworthy events and I usually recover within a day or two and spend perhaps a day in bed max. Colds I pick up from time to time, cough, sore throat, possible runny nose, may be swollen glands in neck but nothing that would confine me to bed or stop me going out for a walk.
Spot on. I’ve had two bouts of real ‘flu in my life – one the notorious 1958 virus – and I wouldn’t wish it on anyone.
Viruses can be very nasty – but it’s the overall impact that is relevant in public health terms, and SARS-CoV-2 is nowhere near that 1958 real epidemic.
My experience in a nutshell.
As others have said, flu just wipes you out. Yes, there’s probably a sore throat and a runny nose and feeling lousy as a consequence too, but you never remember that part of it. It’s simply being unable to get up and do anything long past the point where you feel you can put up with this until you get better.
Early 1986 for me, aged 24 and living alone. Never had anything like it before, and certainly never since.
This is a good comparison. You see a £20 note on the pavement outside your house. If you’ve got a cold you will dash out and pick it up. If you’ve got flu you will say to yourself ‘ sod it’, ignore it and lie down again.
I have only had flu twice in my life. The last time I couldn’t even stand up without passing out for several days and just lay in bed delirious feeling I was about to die. It is really nothing like a cold.
I’ve never felt that I’ll, at least not by contracting a virus.
Funnily enough while waiting for a haircut a couple of weeks ago, the owner, who insisted I wore a face mask (for business compliance reasons) said exactly the same thing (feeling he was about to die) after catching covid and convinced he would have, had he not been vaccinated at least twice.
I have had many bad colds that made me feel awful, but I recall having flu only once and there was indeed a marked difference and, yes, I remember the month and year.
I felt abysmal for a few days, really floored, and I felt wiped out for months – long flu, lol.
Agreed; “flu ( as well as “man ‘flu” ) rendered me incapable of doing anything for several days; Had it twice in 5 decades, but said I have had “the “flu” often ( because I am male…) when in reality it was a bad cold; both times bed ridden, massive drop in energy levels, bad hallunicinatory fever for a couple of days, very bad headaches and body aching all over – drank loads and my system pissed “it” out. Stopped taking ‘Flu jab – tail on the donkey treatment – and upped vitamins and mineral intake.
You’re absolutely right. The human body is a self-healing organism and the symptoms which modern medicine seeks to correct (i.e. suppress) are often the mechanisms through which the healing takes place. Which is why the ‘vaccines’ don’t make sense: why would you want to suppress the symptoms that are in fact healing?
Most medics aren’t doctors either. They’ve never done academic work that constitutes a “contribution to knowledge” in their whole lives.
Many of them can’t even write except in arse-coverese, let alone understand basic laws of causation and how to apply them.
Most of them are charlatans.
Ah. Now, spending time resting and recovering from minor illness means you might not be able to work, so not profitable for your employer and the state. The ideal state of health in their eyes is one in which you’re just about well enough to keep on working while scoffing down all the overpriced medication they recommend, regardless of what it does to you. It’s also partly why tobacco hasn’t been completely banned and in the uk we’re told to drink tap water even though it’s full of nasty stuff. And why antidepressants are dished out like sweeties. And why no one is interested in why everyone is low on vitamin D. Hive management, as they say…
If you read “The Great Cholesterol Con”, “Doctoring Data” and “The Colt Thickens”, I think you may have a better informed understanding when (some, not all) Doctors talk complete bollocks; difficulty is having the balls to raise it with them (I originally typed “confront” – then thought as a breed , sweeping statement but essentially true, Medics are extremely unwilling for whatever reasons to accept their knowledge fallibility) I have done so on several occasions in recent times (all GPs) and none, repeat none (all ages and both non woke genders) were willing to revisit their very apparent unquestioning acceptance of issues such as BMI/Cholesterol/Statins/NICE BP red lines/Salt intake/saturated fat…etc. One GP repeated several times that she was not “a partner or researcher” when I questioned her stance on “vaccines”, particularly supporting the “mandate” type advice to inject very young children……another refused to acknowledge that employing a fully qualified/trained Nutritionist would help their Practice – ” we have a Nurse Practitioner who does that role “; said NP is clinically obese, visibly heavier than I, and has very obvious water retention/Cellulitis type issues. And these are the people representative of some of those who “deliver” a vital part of the… Read more »
I am grateful for the graph and work that went into it, but we will still be discussing graphs this time next year. It is tyranny by numbers, by ephemeral trends, which makes a socio-political breakthrough impossible, and gov tyranny endless. Collecting, monitoring, and especially publishing, statistics has been one of the biggest mistakes of this entire situation, from an objective point of view; and one of the coups of government policy. Governments claimed the virus was a black death deserving of fear and panic (justifying limitless obedience), yet simultaneously allowed the public to view and follow the ostensible progress of the disease like voyeurs and consumers (thus making people ‘own’ and ‘domesticate’ or ‘appropriate’ the horror). So which was true, black death or fun bourgeois spectator sport? And why wasn’t propaganda and censorship used to never talk about the disease and put out positive information downplaying it, instead? Because the virus and situation had to be lethal and homely all at once: sealing off the covidian thesis from attack and penetration. This sharing of death stats, virus progress reports, normalised fear, normalised unthinking acceptance of government data, and normalised the perpetual nature of the ‘crisis’. ‘Democratising’ access to such… Read more »
Agreed. ‘Tyranny by numbers’ = a good soundbite for one of the libertarian MPs (Tory right, Labour left, Lib.Dems etc) to use in their next speech.
It was a cruel and terrifying bourgeois spectator sport for the weak and gullible (the majority). Rather like forcing people to witness the executions of friends and relatives. Naturally there are perverts who enjoy such spectacles.
“Funds for favours” (Guardian). “Wallpaper for access” (Times). Next it will be teacups for questions, perhaps followed by envelopes for lunches. C’mon, MSM editors. Show us the depths to which you can drop. Would the mainstream British media use similar ludicrous terminology to report corruption in Thailand, Italy, Russia, Belgium, either of the Korean republics, the United States, France, Germany, or even Ireland? Of course they wouldn’t. They’d call corruption corruption. They just don’t want to give the natives at “home” any backing for saying that the British state is corrupt, rather like every other state in the world. That would be tantamount to encouraging the natives to have insufficient respect for their “betters”. And that absolutely would not do. So yeah yeah, someone pasted up some wallpaper or sent somebody else the bill for it, or received a cheque for it… Right. Let’s get a lord or a lady to straighten their back and call in some papers and ask some questions. After all, must keep the country squeaky clean, eh? Especially a country where the leaders of the two main “opposition” parties are not only “privy counsellors” but also “knights”. With any “important” “inquiry”, it always seems to… Read more »
Bad news for bedwetters and Branch Covidians. What will they do?
Wet the bed and worship Covid.
Quick, bring out the new variant !!!!!
“Cases of influenza, respiratory syncytial virus and community acquired pneumonia are all substantially below expected levels for this time of year.”
Could that be because most of the elderly in care homes who would normally be expected to be suffering from influenza this year were murdered in 2020?
A very good point indeed, and it looks like they may have been planning to do the same thing again with fresh orders for Midazolam placed..
Even to the convinced and the terrified if they bring out another scarient they will begin to see the whole thing for what it is.
Take Drakefords furious attack on Johnson, the spot light is on him and he tries to deflect it. Like Berkow, he’s going to find himself on the wrong side of history.
Its strange how in the most locked down places, Wales and Scotland, its not tailing off, allegedly
The authorities in those benighted areas would scam a grant out of anything, and then stand there looking baby-faced as they try to scam further grants that are even bigger.
The “pandemic” has been Christmas every day for them. This is particularly so in Scotland, where the fascist local authorities
E-mail the Welsh First Minister. Easy to find his address or that of anyone else in the Welsh government.
Even better, if you have an address in Wales, state that you plan to move your business to England if the persecution doesn’t cease.
Scotland: the military has been called in to “help with the omicron crisis”. Imagine if something real happened!
Meanwhile the Independent reports that “NHS leaders (have been) accused of ‘bullying’ hospitals into silence over scale of Covid crisis“.
Is there a word for that kind of propaganda, where the real state of affairs is X, you get someone to say it’s a million miles from X, and then you blame them for saying it’s so close to X?
Sometimes “a million miles from X” can be portrayed as an extreme goalpost, as you create an argument over whether the distance from X is a million miles or a trillion miles.
There’s an increasing amount of this about.
Certain actors have specialised in it for quite some time – and not just on “Wikipedia”.
The crisis has been caused by the testing.
Its almost like these curves flatten themselves without the need for nation destroying lockdowns?
A pandemic of the tested
Thank you for the analysis, much appreciated as usual. On a completely unrelated note, I happened to stumble onto a paper on PubMed yesterday, providing a balance sheet for the cost/benefit of implementing a measles vaccine program in Pakistan. I was extremely impressed by the simple balance sheet style of summing up ‘adverse events in unvaccinated’, ‘adverse events in vaccinated’ ‘risk difference’, ‘number needed to treat’ and then the overall benefit. Brilliant, exactly the kind of thing I would like to see for covid. But, what shocked me, was not that death rates were as high as 15% in undeveloped countries, with an obvious benefit to vaccination, but the 0.000something% risk of death in unvaccinated in developed countries. When looking at the individual adverse events, it turns out that the biggest risk of measles is actually diarrohea, which of course makes dehydration the key difference between death rates in developing and developed countries. It is stunning that we have a well established measles vaccination program in a country, where not only the Number needed to treat is well in excess of 1000, but where simple clean water and sanitation has made the biggest difference to surviving measles. How much more… Read more »
Isn’t it high time to revive the point that no such thing exists as asymptomatic transmission of cvd19. How have the covid fanatics got away with maintaining its existence for so long in the absence of a single authenticated case? No acute respiratory virus in the past has ever been transmitted by people who were not already coughing and sneezing, and no evidence exists for believing sarscov2 is any different.
Having spent a night with next to no sleep, sweats, shivering, headache, etc. I’ve just taken a test and am positive! Hurrah. I feel fine now. I really feel I should post the test result on social media along with the usual “think how much worse it would have been if I’d not been vaccinated!” blurble. I wonder how many of my online friends would guess that I haven’t had the clotshot?
Oh yes, and I’m pretty certain I had the “proper” ‘vid back in November 2019, along with about half my office.
Post this photo of your test results:
Ouch, full cunt, hope I never catch it.
Excellent update as always!!!
One bit in that is very important:
It is worth remembering that the common cold is responsible for a number of cases of ARDS every year — ie, the same thing as ‘severe covid’ (and closely related to sepsis). We don’t know exactly how many cases as we don’t have everyone testing themselves for ‘having a cold’ all the time.
ARDS is rather common (estimated at about 10% of ICU admissions pre-covid); have we reached the point where we’re seeing normal background rates of ARDS given that we’ve got a rather large number of people ‘with a bad cold’ at the moment?
Dear Doctor,
A big thank you for all your effort to bring these updates to us. You help keep us sane.
Julian
Where has flu gone, even a cold, lots of vaccinated now have covid, apparently, no colds or flu. If you test negative is it a cold?
This sums it up I believe.
Lolism!
From Jon Rappoport:
On December 29, the head of the CDC, Rochelle Walensky, announced, in a White House press briefing, that the PCR test can register positive (meaning the person is “infected”) long AFTER infection is over.
Here’s Walensky’s money quote:
“…people can remain PCR positive for up to 12 weeks after infection and long after they are transmissible and infectious.”
There’s your ‘long covid’ and ‘incidental infections’ done away with. All PCR-based bullshit.
Stole this from a poster on The Telegraph’s site.
‘Guardian winter headlines 2012 – 2019:
2012: Hospitals ‘full to bursting’ as bed shortage hits danger level
2013: Hospitals scramble to prevent crisis in NHS’s ‘toughest ever’ winter
2014: More patients, overstretched doctors – is the NHS facing a winter crisis?
2015: Hospital bed occupancy rates hit record high risking care
2016: Hospitals in England told to put operations on hold to free up beds
2017: NHS bosses sound alarm over hospitals already running at 99% capacity
2018: NHS intensive care units sending patients elsewhere due to lack of beds
2019: Hospital beds at record low in England as NHS struggles with demand’
Excellent find.
Anyone with access to Grauniad editions pre 2012?
Idle curiosity as I’ve heard that even if the NHS got 100% of GDP until the heat death of the universe it would still be struggling to cope.
Great. They would claim, however, that the recent ‘crises’ were for a black death, not just ‘normal’ diseases. Bloody liars!
Why would anyone be surprised that Whitty is wrong again?
He’s the government’s Chief Scientific Charlatan.
Let’s call your in house Doctor, Dr Sanity. Let’s put him or her in charge of the NHS. Of course being a good doctor he/she wouldn’t want to join the ranks of the medical meddlers and bureaucrats. These people are killing the NHS and compromising healthcare through their insane policy responses, sure Dr Sanity wouldn’t want to join their closed ranks. In any case the manifest humanity and patient centred perspective wouldn’t get through the interview panel. The NHS leadership is the sickness.
I’ve made a plot of the English population by age showing what proportion have had one, two, three doses of the experimental vaccine or have avoided the poison. It’s based on the UKHSA figures.
Encouraging that the majority of the population haven’t had 3 doses.
And in the older age groups (above about age 60) there are roughly as many who have stuck at 2 doses as there are unvaccinated in the same age groups. So the ‘not fully vaccinated’ have roughly doubled in those older age groups.
And looks like the triple vaxed in those older age groups have levelled off so hopefully those number who have stuck at two jabs will not diminish materially.
What proportion according to whose estimate of the population?
For under 18s and people of pension age I reckon the state has a pretty good idea of how many people there are. Between 18 and 66/67? They’re guessing.
It’s based on the NIMS database as used by UKHSA (number in NIMS who are unvaccinated divided by total number in NIMS).
There are many reasons based on indirect calculations to believe that the proportions aren’t far off the mark, even if the absolute numbers may not be spot on. But yes there is some uncertainty.
Sorry, correction to chart (error in 30-49 ranges)