Pressure Mounts on the UKHSA to Stop Publishing Data Showing Infection Rates Higher in the Vaccinated
The Prime Minister may have acknowledged reality and stated that being double vaccinated “doesn’t protect you against catching the disease, and it doesn’t protect you against passing it on” but others appear to remain in denial.
On Sunday I asked whether now that the PM had let the cat out of the bag the media would start reporting properly on the UKHSA data showing higher infection rates in the vaccinated than the unvaccinated. It appears the answer is no, at least if the Times‘s Tom Whipple is any indication.
In a typically mean-spirited piece – in which anyone who doesn’t agree with his favoured scientist of the hour is smeared as a conspiracy theorist and purveyor of misinformation – Whipple quotes Cambridge statistician Professor David Spiegelhalter, who heaps opprobrium on the U.K. Health Security Agency (the successor to PHE) for daring to publish data that contradicts the official vaccine narrative. Spiegelhalter says of the UKHSA vaccine surveillance reports:
This presentation of statistics is deeply untrustworthy and completely unacceptable… I cannot believe that UKHSA is putting out graphics showing higher infection rates in vaccinated than unvaccinated groups, when this is simply an artefact due to using clearly inappropriate estimates of the population. This has been repeatedly pointed out to them, and yet they continue to provide material for conspiracy theorists around the world.
This is the graphic he is presumably referring to.
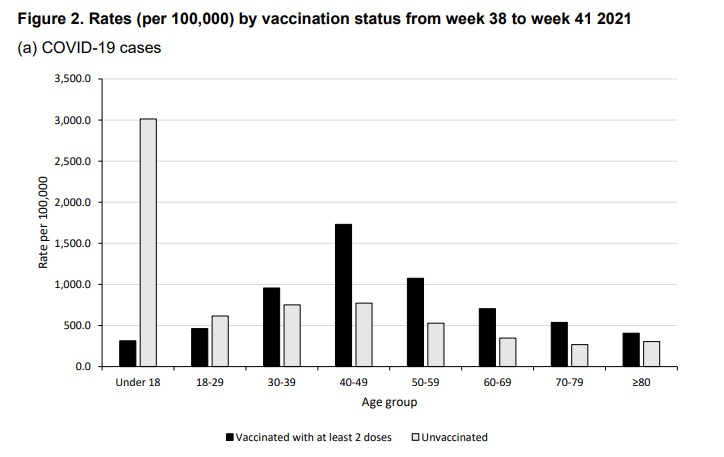
If Professor Spiegelhalter has a source for his claim that higher infection rates in the vaccinated are “simply an artefact” of erroneous population estimates then he doesn’t provide it.
Whipple says the data has been “seized upon around the world”.
The numbers have been promoted by members of HART, a U.K. group that publishes vaccine misinformation. They have also been quoted on the Joe Rogan Experience podcast in the US, which reaches 11 million people.
Appearing on that podcast, Alex Berenson, a U.S. journalist now banned from Twitter, specifically referenced the source to show it was reliable.
The UKHSA is adamant that it is doing nothing wrong. The Times quotes Dr Mary Ramsay, head of immunisation at the UKHSA, explaining: “Immunisation information systems like NIMS are the internationally recognised gold standard for measuring vaccine uptake.”
So Professor Spiegelhalter thinks that the gold standard gives “clearly inappropriate estimates of the population”, and using it is “deeply untrustworthy and completely unacceptable”? That may be his view, but the UKHSA can hardly be criticised for following the recognised standards for its work.
A more measured criticism is provided by Colin Angus, a statistician from the University of Sheffield, who the Times quotes saying that using NIMS data makes sense but the “huge uncertainty” in the population estimates should be clearer.
Whipple, however, goes further and claims that “using population data from other official sources shows, instead, shows that the protection of vaccines continues”. Yet he does not provide those sources or go into any detail about how they back up his claim.
For now, the UKHSA is defending its report (we’ll see how long it holds out for). But even so, Dr Ramsay is adamant that the report rules out using the data to estimate vaccine effectiveness: “The report clearly explains that the vaccination status of cases, inpatients and deaths should not be used to assess vaccine effectiveness and there is a high risk of misinterpreting this data because of differences in risk, behaviour and testing in the vaccinated and unvaccinated populations.”
This defence somewhat misses Professor Spiegelhalter’s criticism about population estimates. But it’s also misleading in that the report doesn’t “clearly” explain that its data “should not be used to assess vaccine effectiveness”. What it says is it is “not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation”. But, as explained before, using population-based data on infection rates in vaccinated and unvaccinated is certainly a valid method of estimating unadjusted vaccine effectiveness, which is defined as the reduced infection rate in the vaccinated versus the unvaccinated. While a complete study would then adjust those raw figures for potential systemic biases (with varying degrees of success), we shouldn’t necessarily expect those adjustments to be large or change the picture radically. Indeed, when a population-based study from California (which showed vaccine effectiveness against infection declining fast), carried out these adjustments the figures barely changed at all.
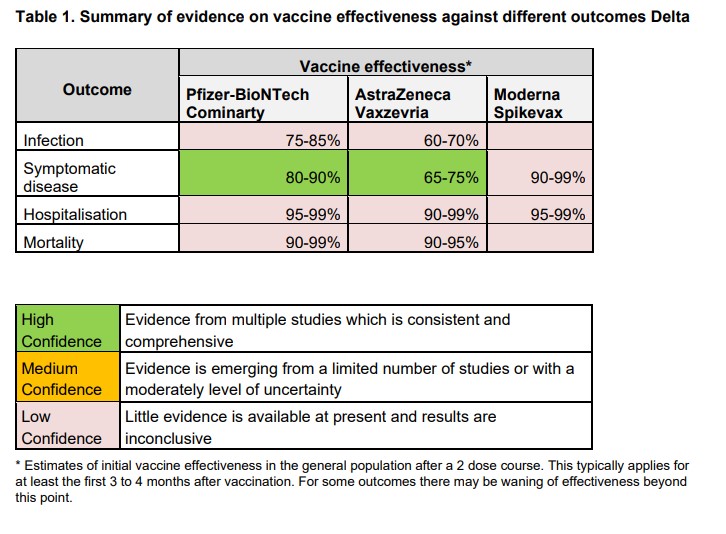
The UKHSA report adds: “Vaccine effectiveness has been formally estimated from a number of different sources and is described earlier in this report.” In fact, though, most of those estimates are reported as low confidence (see below), which means: “Little evidence is available at present and results are inconclusive.” While it claims high confidence for its estimates against symptomatic disease, a footnote explains that this only holds for 12-16 weeks: “This typically applies for at least the first three to four months after vaccination. For some outcomes there may be waning of effectiveness beyond this point.”
It is precisely this “waning of effectiveness” that the latest real-world data is giving us insight into. Rather than trying to discredit that data and those who report it by throwing around general, unquantified criticisms, scientists and academics like Professor Spiegelhalter should be redoubling efforts to provide constructive analysis to get to the bottom of what’s really going on with the vaccines. If there are issues with the population estimates then those need to be looked at, and if there are biases that need adjusting for then those need to be quantified. But do, please, get on with it – and lay off the smearing of those who raise the questions.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I suggest checking where the prof gets his funding…..
Just how far wrong can the population estimate be?? Surely not enough to materially alter the outcome? In any case, I can only see the ‘real’ number being higher than official estimates. And of course, this would do nothing to hide the clear trend in this data that Will has pointed out in recent weeks.
UK population must be one of the best documented in the world unless they really have lost all control of immigration.
Does the new acronym UKHSA mean that Wales, Scotland and N.I. have lost their independent Agencies and, if so, what is the relationship between UKHSA to the devolved administrations?
That is a good point. Being PHE’s successor also implies that it’s also the successor to PHS, PHW, etc. Coupled with the fact that health outcomes are rapidly taking over as the number 1 consideration in policymaking, UKHSA in fact wields an extraordinary level of power and influence.
Just as bodies such as Homeland Security in the US and counter-terrorism units in many countries increased their control in the wake of a succession of terrorism incidents starting with 9/11, now a similar trend is occurring with the public health bodies. But the merging of the UK’s four previously independent agencies into the UKHSA could be a particularly pernicious development, because it could mean that, in parallel with this, there is also an increase in centralization of control, where new “official advice and guidelines” are applied UK-wide regardless of each country’s local circumstances.
Nah. Look forward to the new figures from the census.
And remember even so that large numbers of people are not reported on the census … criminals, obviously, anyone packed unlawfully into a council flat, or unlawfully in private flats, all illegal immigrants.
Not that that supports these objections. A very big confounder is what proportion of the vaxxed and unvaxxed are naturally immune … something they seem strangely unwilling to check.
The natural immunity of the population is something that hasn’t being addressed very well during the emergence of Sars-Cov-2 during the last couple of years. I would think that at the present time the vast majority of the population have in one way or the other been exposed to it, and consequently the ((conspiracy theory)) immune response has taken note rather like the Police build up a dossier of possible trouble makers in a particular area – Or should do !
I recon the background exposure like Grandchildren, Super Market’s and Trolleys, handling the Mail without disposable gloves and disinfectant, forgetting to Wash Your Hands occasionally or singing Happy Birthday BORIS, etc. is the most important and will result in a robust immune response without you really noticing other than occasionally the “Sniffles”.
At the other end of the of the exposure spectrum would be the Front Line Workers with high pathogen loads, in which case OUCH that hurt!!!
Actually, in age groups where most people are vaccinated, the calculation of vaccine effectiveness is very sensitive to small differences in the population estimate.
We know quite accurately how many people have been vaccinated. The number that are not vaccinated is calculated by taking the number vaccinated away from the population total.
Suppose you estimate the population to be 1,000 and 950 have been vaccinated – then you would calculate 50 are not vaccinated.
But if you estimate the population to be 5% larger i.e. 1,050, then you would estimate that the number unvaccinated is 100 i.e. double.
As the vaccine effectiveness is proportional to the unvaccinated population this can make quite a difference.
MHRA uses the NIMS method of estimating populations which is acknowledged as probably being an overestimate.
For the 40-49 age data they’d need to reduce the population estimate by about 10% to get the vaccine effectiveness back above zero.
I am not saying that population estimation is the only problem. Just that it can make a big difference.
There is something odd about that age group – the vaccinated infection rate is consistently much higher than any other group older or younger. In fact the vaxx rate seems to rise to a peak in that group and drop away as you get older or younger. There is no such tendency in the unvaxx group.
It has nothing to do with age per se, rather the time elapsed since that cohort had their injections. They started with the elderly and worked their way down, so the older you are, the more time your jabs have had to become ineffective.
That makes sense. What doesn’t make sense is that the Technical Briefings have been going since April or so. Yet Spiegelhalter has waited until now to claim the data is corrupt? That is a red flag for me.
I bet he’ll claim a million unvaccinated migrants are landing every day, if it’ll help his attempt to beef the numbers of the unclean
What is your basis for saying that the PHE calculate figures for the number of not-vaccinated as the population less the vaccinated total in working out their ‘cases’ per 100,000 etc?
For example what if they cross-check each ‘case’, hospitalisation or death against the vaccination status whether vaccinated or unvaccinated? Perhaps there are duplicate records of some of the population, and the matching happens with the closest matched record. They then apply the proportion of unvaccinated/vaccinated from this matching exercise to the numbers in their database.
Surely it is then possible that they get the total population wrong (too high) while either over-estimating or under-estimating the unvaccinated proportion?
What is your basis for saying that they calculate figures for the number of not-vaccinated as the population less the vaccinated total?
It is the standard way of doing it (sorry can’t find a reference right now – but will dig around when I have more time). Can you think of an alternative?
For example what if they cross-check each ‘case’, hospitalisation or death against the vaccination status whether vaccinated or unvaccinated?
That will tell you how many people who are hospitalised/dead were not vaccinated. But it doesn’t tell you how many people were not vaccinated and were OK.
I’ve not seen anything that explains their methodology, so if you can find a reference to show it’s the ‘standard way’ then please post. Until you do we must take your assertion as not yet verified On the second point, I don’t think you understand what I’m saying, maybe I wasn’t clear enough. Imagine there are 60 million records on a vaccination status database for a 56 million population. And that’s because there are 4 million duplicate records. And when a positive test happens they go away and check against that 60 million database for the nearest match. And keep a record of all these positive tests and sum them up. And they then calculate the unvaccinated case rate per million as the total of all positives matched to an unvaccinated record on the database divided by the number of million of unvaccinated people recorded on the database. And they calculate the vaccinated case rate per million as the total of all positives matched to a vaccinated record on the database divided by the number of million of vaccinated recorded on the database. Now if say all 4 million duplicates on the database are of double vaccinated people. Then you… Read more »
But surely our problem is that we effectively don’t know the size of the database?
You started by asserting Actually, in age groups where most people are vaccinated, the calculation of vaccine effectiveness is very sensitive to small differences in the population estimate.We know quite accurately how many people have been vaccinated. The number that are not vaccinated is calculated by taking the number vaccinated away from the population total. I asked ‘What is your basis for saying that the PHE calculate figures for the number of not-vaccinated as the population less the vaccinated total in working out their ‘cases’ per 100,000 etc?’. You asserted “it is the standard way of doing it (sorry can’t find a reference right now – but will dig around when I have more time). Can you think of an alternative?” I provided a more plausible alternative but in no way assert that the alternative is correct merely more plausible. Do I take it you have no reference for your assertion, because you clearly have plenty of time. Norman Fenton (etal) set out in their paper why it is likely that the proportion of the population who are unvaccinated is likely to be understated and asks for the data from the ONS to check whether this his conclusion is right… Read more »
We know the implied size of the English population from the Vaccine Surveillance Report by working back from the numbers of cases and the case rates per 100,000 and we can estimate the partially vaccinated from the vaccinated to date percentages Mode RNA above has done the sums, and that gives about 22m unvaccinated, 38 million double vaccinated and 3 million partially vaccinated. So 63 million total English population vs the ONS estimated mid-year population estimate of about 56.5 million in mid-2020 for England which probably hasn’t changed much this year. So about 6.5 million more than the ONS population estimates. If the vaccinated number is right and the English population is around 56.5 million in practice (perhaps the recent census may give us a good estimate), and the unvaccinated is worked out by subtraction of the vaccinated from the total population as you conjecture, then the unvaccinated have been underestimated by about 6.5 million (really 28.5m not 22m) Using your conjecture of unvaccinated are the difference and vaccinated number right would reduce efficacy figures for cases, hospitalisations and deaths, roughly speaking, unless the correct population was more than 63 million. Of course the effect will depend on the age… Read more »
We can roughly deduce the size of the NIMS database. It’s about 63 million. Roughly speaking. And that’s all those registered with a doctor in England (including records that shouldn’t be there and duplicate records etc)
22 million unvaccinated
38 million double vaccinated
3 million partially vaccinated
(mode RNA did the sums earlier you can work back from the PHE UK HSA figures based on case numbers and cases per 100,000)
And perhaps the English population is 56.5 million (the census might give us a better estimate).
So there are perhaps at least 6.5 million more records than should be on there. It’s probably more because of those not registered with a doctor.
So our real problem is where are those 6.5 million or so records that shouldn’t be there coming from? Are they duplicate records? Are they people who have changed practices and are on for both practices. Does it include some people who have now left the country before or after getting vaccinated.
And how do we account for people who aren’t registered with a doctor or become newly registered with a doctor.
You are just tilting at windmills. Use the ONS figures if you want, which are acknowledged as an overestimate. Or somewhere between the two. It makes no difference: the rate in the vaccinated is of the same order as in the unvaccinated whichever figures you use, whereas with a real vaccine it would be orders of magnitude lower. That’s the issue. Alternatively, by your own admission, the rate amongst the vaccinated population is known because we know how many are vaccinated. Fine. Compare the rate in the vaccinated 40s age group with the rate in the unvaccinated earlier this year when the take up of the vaccine in that age group was such that 50% were unvaccinated. Or take a look at the 30s age group, where even today vaccine uptake for a first dose is less than 75% (i.e. 25% unvaccinated). The argument about uncertainty in a residual or difference becomes pointless when the unvaccinated constitute around a quarter of the population: it matters little whether that population is in reality 23% or 27%, the rate estimate will still be within +/-10% of the true figure. Go on. Be my guest. Push up the rate in the 30s age… Read more »
MTF, like Spiegelhalter, is desperately hunting for ways to rationalise what he desperately wants to be the truth. As so often through this covid panic, this has resulted in such people hunting out ever smaller effects and issues with data, and trying to pretend those justified their support for disastrously costly panic responses. But the reality is that if the data came even close to supporting the catastrophically costly panic response they fell for, there would be no need to hunt around for tiny “proofs” buried in the data. We’d see huge and obvious effects in the different responses around the world. for lockdowns, for mask mandates, for vaccinations etc. The desperation of their searching already defeats their core position, but they will never admit it. The covid conversations have gone roughly like this: Panicker: “WE’RE ALL GOING TO DIE IF WE DON’T LOCKDOWN/MASK UP/VACCINATE etc” Reasoning sceptic: “Calm down a moment. What’s the evidence for this?” : [Society runs around in a headless chicken response driven by media pushing of panicker lines and nefarious political and corporate opportunists jumping on bandwagons] Months or years later: Panicker: “So as you can see from this detailed and complex statistical analysis that… Read more »
“... the reality is that if the data came even close to supporting the catastrophically costly panic response they fell for, there would be no need to hunt around for tiny “proofs” buried in the data.”
Yes – I’m totally sick of the busting of the gut to justify the irrational, in the face of a mountain of real evidence.
They succeed by obfuscating the huge reality beneath a pile of trivial details.
Instead of the debate being about asking where their false predictions of disaster went, and why we spent so much and inflicted so much suffering and injustice supposedly trying to avoid it, it’s about how precisely the data should be manipulated and corrected to make it a few percentage points more supposedly accurate.
https://www.babelmatrix.org/works/de/Morgenstern%2C_Christian-1871/Die_unm%C3%B6gliche_Tatsache/en/32691-The_Impossible_Fact
very good!
Indeed, the same is true in spades of the “climate emergency”, which as far as I can tell consists of media reports of bad weather (never good weather) presented completely out of the context of the weather history of the region concerned, as though they had never happened before. Sometimes extreme temperatures get a small nudge from urban heat island effect as populations expand, pushing temperatures into “record” territory; we saw this in the heatwave in northwest USA a few months back even though similar heatwaves have happened there every few decades. If that’s the best evidence they can scrape together, it suggests that the case for the “climate emergency” doesn’t exist.
I reckon you are right; an apologist for “vaccines” when it has been confirmed – by one manufacturer at least – that they are a gene editing therapy – but then in this chimeric world, “something can be anything you want it to be”. How many more times will this misguided ….person….try to deflect and dissemble before the real world nasty hard facts hit home I wonder.
MTF:
Please list the ENTIRE list of ingredients of the Pfizer original, now renamed Cominarty, jab;
Please confirm, to your knowledge or opinion, with cited references, that the S1 spike protein stays at the injection site “for a few days only” as you stated recently.
What version of the S1 spike protein is induced with the current booster jabs and how many other antigens are not targeted
And these are just a few of very difficult aspects of this entire charade you seem content (or desperate) to gloss over – “can you find references to the above or alternatives ?”
Very predictably silent.
Tilting at windmills is right. They’d have to hide the numbers of other countries as well.
Dutch health authority has been keeping track of infection rates in jabbees/non-jabbees since August. August saw around 67% of infections in non-jabbees (primarily school children). September saw a slight increase in jabbee infections, October saw a higher increase, which is still going up. Last week 44% jabbee infections, 56% non-jabbee. This week 47% jabbee, 53% non-jabbee.
Even taking account of a lower number of non-jabbees (almost 90% jab rate in over 50s), the trend is clear. At some point the non-jabbees will have all had the virus, while jabbees will keep getting infected. The numbers are percentages of the actual infections in a given week, but the direction is obvious and following the route already laid out by Israel and the UK.
What effective prophylactic requires an incredible train of re-jabbing in the vague unscientific hope that more snake oil=success?
But the snake oil is successful, wildly so.
There is categorical, highly scientific proof that the snake oil has raked in billions upon billions for pfisser, with zero liability, zero need to actually prove effectiveness or safety and an incredible ability to pretty much wipe out anything resembling competition. The biggest success has been in keeping out any competing therapeutics that might show this stuff up for the snake oil it is (actually, I suspect actual snake venom would be less toxic).
Oh wait, you were talking about the success of the product for the millions of people receiving it? Well, they may still get a cold, but possibly maybe perhaps not suffer so much from it – or maybe they might.
Use the ONS figures if you want, which are acknowledged as an overestimate. Or somewhere between the two. If they are also an overestimate, I don’t see we are any better off? It makes no difference: the rate in the vaccinated is of the same order as in the unvaccinated whichever figures you use, whereas with a real vaccine it would be orders of magnitude lower. My point is that where the vaccination rate is very high we don’t really know the rate in unvaccinated using this method because it is too sensitive to population estimates. So we can’t say they are of the same order of magnitude. However, for other reasons, I absolutely accept that vaccine efficacy against infection is declining – I just don’t think the MHRA reports give you a good handle of how much they have declined. “Real vaccines” vary a lot in their efficacy – flu vaccines can be very low – of course you can always define “real” as meaning “has very high efficacy”. Alternatively, by your own admission, the rate amongst the vaccinated population is known because we know how many are vaccinated. Agreed. Compare the rate in the vaccinated 40s age group with… Read more »
”Can we keep the dialogue polite and respectful?”
Doubtful.
Mainly because of the conduct of those who have the unshakable belief of the zealot in their conviction that, despite being made by convicted felons, the ‘vaccines’ are of such inestimable benefit to every human (as if they are identical clones) that they must be ‘vaccinated’.
I’m afraid that respect and politeness were the first casualties in this war for bodily integrity.
Utter nonsense.
They are the same order of magnitude whether you double the rates in the unvaccinated.
Now you are not only tilting at windmills, you are clutching at straws.
It is disingenuous to turn the matter into an argument about precision or absolute accuracy of the rate (‘we don’t really know the rate in unvaccinated’) when the rates are clearly of the same magnitude now (whichever population estimate you take, whether the overestimating one or the underestimating one) and no vaccine benefit in respect of infection can be claimed with any statistical significance, as admitted by the manufacturer Pfizer themselves to the FDA on September 17 (‘not statistically significantly different from zero’).
They are the same order of magnitude whether you double the rates in the unvaccinated
Well I guess it is a case of what you call “same order of magnitude”. If rates appear similar but the unvaxx rate might be double your estimate then that strikes me as pretty significant.
no vaccine benefit in respect of infection can be claimed with any statistical significance, as admitted by the manufacturer Pfizer themselves to the FDA on September 17 (‘not statistically significantly different from zero’).
Benefit when? Most people have accepted it has declined and might currently be very low. There was a very significant benefit when the vaccines were first given.
Anyhow, my main point remains. The MHRA stats are not very useful for estimating efficacy.
There you go again.
Absolute efficacy maybe (i.e. whether it’s now -10% or +10%).
But perfectly good enough to show that the vaccine efficacy is shot to pieces.
I don’t think we disagree that much. I accept, along with most people, that the efficacy against infection of all three vaccines declines sharply about five months after the second injection. We don’t need the MHRA stats to prove that. Whether you call this “shot to pieces” or not is more of an emotional things than a data/stats thing. At first glance the MHRA stats might give us more information on vaccine efficacy such as exactly how much have the vaccines declined and how does this vary among age groups. I have presented some reasons for doubting whether they are suitable for this task. The higher age groups have very high vaccination rates which mean that VE estimates could easily be wrong by 50%. The change in efficacy in the lower age groups seems to be largely down to a change in the unvaccinated rate which doesn’t fit in with it being down to declining VE. Throughout there is no allowance for confounding factors other than age. You can add to this: The sample sizes in the older age groups are extremely small. Your argument seems not to deny these problems but to claim that they can’t sway the estimate… Read more »
“There was a very significant benefit when the vaccines were first given.”
Please confirm how you reach that conclusion; do you mean prevention of infection acquisition, propensity to transmit by symptomatic or prophylactic effect where a person has a detectable viral load and exhibits symptoms of CV19?
How significant is the – initial, by your comment – benefit of these jabs – as far as reducing the more severe effects of CV19 when compared to the early intervention regimes practised in the US, India and elsewhere? When did the UK PHE/DHSC/MHRA/NHS implement the same early treatment regimes; what was the effect on UK ICU hospitalisations of these early treatment regimes.
Very interested to read your forensic response, with unimpeachable references so we can all double check that you are being “sincere according to truth”.
“Can we keep the dialogue polite and respectful? ” Why cannot we keep the dialogue “sincere according to truth” – at the risk of me being repetitive and boring. You have made many statements related to statistics which others with knowldge I do not possess have addressed – I can only take these exchanges at face value because I do not possess in depth knowledge of that element. However I remain deeply sceptical – a massive understatement – when I read something – “X” – which I then find out is substantially less than accurate (that is me being “polite”) or indeed “Y” You have made one outrageously false and utterly disgraceful statement about these gene editing therapies relating to Anaphylaxis – and I posted that you were wholly ignorant of not only that condition but also about the lack of pre EUA testing on individuals who suffer from this. The fact that these jabs can over prime your immune system and induce a cytokine effect is a potentially very deadly consequence and I don’t care a flying **** if you opine that is a “rare” occurrence; if it kills you, “rarity” does not come into it, but it serves to… Read more »
“the rate amongst the vaccinated population is known because we know how many are vaccinated.”
I’m not sure that we can take even that for granted, given the abysmal accuracy of official statistics. It a two-way sword.
Fascinating how Narrative backers like you are suddenly become sensitized to data inaccuracy!
The problem for you is that observational data, government confessions and ARR calculations consistently go the same way in terms of overall efficacy. Time to give up on a lost cause!
So – war cries aside – do you accept that VE estimates are extremely sensitive to population estimates where the vaccination level is high?
Leaving the rather useless timewasting effort on data innacuracies, the only logical position of jabbed to take is to back endless rejabbing every 6 months.
However if the same ‘original’ spike is used in these rejabbings all that will happen is that the rejabbed will get more and more exposed to variants/strains, and possibly very sick or die.
The unjabbed will still have the ability for natural immunity response to new strains. Possibly if it every brought to market the Valneva job might offer the same sort of benefits. However as no government anywhere has preordered it, there is clearly a wish for this not to happen.
This is a pretty good point. Even if one truly believes the pfisser poison is effective in the early months – and it’s not clear how effective it is for how long, as they seem to imply that effectiveness starts dropping noticeably after 2 to 3 months and by month 5 it’s close to useless – that in itself indicates that what was initially touted as a first generation vaxx for corona would appear not to be the best possible.
At this point they should absolutely be looking at other, non-mrna vaxxes to see if they could do a better job. Novavax and Valneva seem to have faded into nothing, in favour of pfisser, which works for a few months at best, has lots of side effects, which could quite possibly acculumate as time goes by – yet they all still insist on going with it. Either those making the decisions have all been bribed or they have taken the vaxx and it really does alter people’s ability to think clearly.
No there is ONE whole virus vaccine in development, Valneva, and its clearly being ignored.
There is every reason to think they will continue to use the same spike. They could stop doing it anytime they wanted, they haven’t.
No jabbed people who get covid will not ‘reap the benefits of anything’. Their natural immune system will have been compromised and the jabs increasingly useless.
Natural immunity does not need ‘developing’ . We all had it before useless jabs were given and are now compromising the immune system.
People who don’t take an annual flu jab are doing fine.
It is impossible for you to be more wromg about this stuff. I would stop digging if I were you and reach for the ladder.
No there is ONE whole virus vaccine in development, Valneva, and its clearly being ignored. Sinopharm and Sinovac are both whole virus. The WHO vaccine tracker has 17 inactivated whole virus vaccines and 2 attenuated live virus vaccines in development. The larger point is that vaccine development and treatments will improve – possibly Ivermectin. So, there is good reason for putting off infection or serious illness now. (Re using the spike protein) They could stop doing it anytime they wanted, they haven’t. It is less than a year since the first vaccines were rolled out. Let’s see. No jabbed people who get covid will not ‘reap the benefits of anything’. Their natural immune system will have been compromised and the jabs increasingly useless. In what sense “compromised”? If you mean the vaccines in some way harm the immune system that is a contentious issue. Natural immunity does not need ‘developing’ . We all had it before useless jabs were given and are now compromising the immune system. I meant developing in the sense of being more widespread. People who don’t take an annual flu jab are doing fine. Some are, some aren’t. The efficacy of the jab varies from year to year… Read more »
No, I don’t accept that at all.
I’m interested in Spiegelhalter’s stance, because I’ve always thought of him as a good statistician. One of his illustrative insights that I recall is rubbishing the misuse of relative risk reduction in the context of eating bacon (the absolute greater risk of cancer being vanishingly small).
However in an article about the age gradient of Covid mortality, he uses precisely the relative risk error that he also condemns (i.e that a ‘doubling of the risk of death between two small percentages is a headline feature)
I think that he is probably a victim of conformity pressures, always trying to say ‘I’m really a good boy’ to the powerful when he fears he might have offended.
The fact that Norman Fenton has been censored and Spiegelhalter hasn’t is indirect confirmation of this.
What seems obvious to me is that the most likely direction of error in population estimates is towards underestimating total population. Given that the vaccinated number is known more accurately the proportion of unvaccinated who are infected is likely to decrease if the population estimate grows, since the error will fall in that sector.
me:do you accept that VE estimates are extremely sensitive to population estimates where the vaccination level is high? RickH: No, I don’t accept that at all. It follows from the maths – does your scepticism extend to the fundamentals of mathematics? Perhaps maths is a lie pushed by “experts”? On Spiegelhalter’s stance. The relevance of ARR as opposed to RRR is dependent on the context (see below*). So that may explain his apparent inconsistency. However, you don’t give the references so it is hard to know. (I think we can assume he is a better statistician than either of us!) * In some contexts the absolute risk is clear and therefore it makes sense to give the ARR. For example, if you get lung cancer then your absolute risk of dying in the next 5 years is well known and the ARR of a treatment makes sense. In other contexts, the absolute risk varies a great deal and therefore the ARR varies a great deal. For example the absolute risk of getting pertussis obviously depends on the time period (is it just the risk of getting it tomorrow or sometime in your life) and the prevalence of pertussis – if there… Read more »
If the unvaccinated cohort is double the estimate, as per your example, that would mean that the injections are even less effective. The number of reported infections stays the same but is taken from a sample pool twice the size, meaning that the infection rates in the unjabbed are even lower.
I am sorry – it is hard to work out which of my comments you are replying to. My point was simply that the estimate of the size of the unvaccinated cohort is extremely sensitive to small errors in the estimate of the population size. This could work both ways. NIMS which is used by MHRA says itself that it is likely to be an overestimate of the population leading to an overestimate of the unvaccinated population leading to underestimate of the infection rate in the unvaccinated.
You might be interested in this https://www.covid-arg.com/post/vaccine-effectiveness-and-population-estimates They are claiming the overestimate of the numbers on NIMS is solely because of the records of people who have left the country are on the system as unvaccinated. They produce this reason with nothing solid to back it up However, it is thought to significantly over-estimate the population because patients aren’t reliably deregistered when they move, for example if they leave the country. The key bit in this is ‘thought to’. Who has thought that? Where is the actual evidence. Have they taken a random sample from the database and checked whether those people are on the database correctly or not and if not why are they incorrectly on the database. And have they analysed positive cases that they have tried to link to NIMS and not found a record. Easier just to think that it is due to a reason that supports your narrative than actually try to find out. So 6.5 million perhaps have left the country and all of their records remain on the system? And that’s the only error? Doesn’t sound convincing. And what happen with people who aren’t registered with a doctor? Are their records on the… Read more »
You might be interested in this https://www.covid-arg.com/post/vaccine-effectiveness-and-population-estimates Yes – thanks – it is very clear explanation of the problem. They are claiming the overestimate of the numbers on NIMS is solely because of the records of people who have left the country are on the system as unvaccinated. They are claiming there is an over-estimate because patients aren’t reliably deregistered when they move for example leaving the country. Patients move within the country and you get duplicate registration. They also die and the registration is not removed. And I dare say there are other reasons patients are not deregistered when they should be. Bear in mind that this doesn’t have to be recent. Someone may have moved ten years ago and still be a duplicate registration e.g. if they rarely visit the doctor. They produce this reason with nothing solid to back it up The key bit in this is ‘thought to’. Who has thought that? Where is the actual evidence. Have they taken a random sample from the database and checked whether those people are on the database correctly or not and if not why are they incorrectly on the database. And have they analysed positive cases that they have tried… Read more »
The strength of using NIMS is that the numerator and the denominator of the case rate per 100,000 calculation come from the same source, and this is not true of ONS estimates.
The difference between the numbers registered with GPs and the ONS English population is estimated at about 2 million.
So even if we make the sweeping assumption that all these people are unvaccinated people who have not deregistered from doctors when they move, for example leaving the country that still leaves us perhaps with 4.5 million on NIMS for another reason that we can’t account for.
My friend who was double vaccinated in England has emigrated to Spain but hasn’t deregistered with his doctor here. So even within the 2 million registered with a GP but not living here we can’t assume all of them have not been vaccinated.
So yes there is some uncertainty because of the gearing effect especially in some of the older age groups where most have been vaccinated. But which way it effects figures is yet unknown.
And the other evidence such as the Norman Fenton paper, which I have read, suggests the ONS proportions unvaccinated are seriously underestimated.
Your second point is really significant. Even if the baseline is wildly incorrect, the *trend* is undeniable.
I think it is widely accepted that the current vaccines lose efficacy over time.
I see (COVID-19 vaccine surveillance report – week 43) that the UKHSA has bowed to the pressure and stopped charting the rates of infection by age group between the vaccinated and unvaccinated.
Nevertheless, they have tabulated the results, albeit with even more caveats and the label ‘unadjusted’. See below.
Still the rate is more than double in the vaccinated for ages 40 – 79, and also significantly higher in the 30 – 39 and 80+ age groups.
The ‘negative efficacy’ continues to increase in most age groups (rate now 232% higher in the age 40s vaccinated), and the small positive vaccine efficacy in the 18-29 age group continues to be eroded.
Professor Spiegelhalter, who last year produced an excellent graph showing that age mortality rates from Covid-19 closely followed those of normal age mortality, should look at what’s happening on the ground.
The number of double jabbed that I know of personally, who have since “tested” positive for Covid-19, has now increased to 10 compared with only 2 people last year, before the jab made its appearance.
That’s a five fold increase in statistical terms!
This interview of Del Bigtree on the Pandemic Podcast is excellent and explains much of the what is happening and is likely to happen to the jabbed.
https://odysee.com/@pandemicpodcast:c/delbigtree:4
Re. Spiegelhalter – I may have been a bit harsh about his adherence to the Narrative. He has done some interesting work, but I think I’ve noted this tendency to go along with the exaggerated significance of Covid, with some really odd historical analyses.
His article on the age/mortality profile is interesting, although he plays fast and loose with relative risk :
https://medium.com/wintoncentre/how-much-normal-risk-does-covid-represent-4539118e1196
In a sane, well functioning democracy, this data would be front page news for days on end. But we left that world behind in spring 2020.
Oh, the irony. Given that the British public has been fed and swallowed highly questionable data for the past eighteen months plus it’s a bit rich to start complaining about how the government presents figures now.
The ONS was pretty good until they were got at sometime late 2020.
The surprising thing would be if they didn’t bury or twist the information that didn’t fit their plans. They’ve done it with the risk of the virus, the effects of lockdown, the efficacy of masks, the dangers of their jabs, the risk to children and on and on.
You cannot hope to bribe or twist, thank God! the British
journaliststatistician. But, seeing what the man will do unbribed, there’s no occasion to.Dr Clair Craig has several tweets on how PHE and ONS often ‘fudge’ the numbers…
this is another..
PHE’s measurement of the English population keeps growing. People with no NHS record come forward to be jabbed and get added to the total.
In Scotland there are always, always 5,915,448.
When someone new comes forward, one of the unvaccinated with a record just disappears.
https://twitter.com/ClareCraigPath/status/1451220104100917248
Also
Proffessor Norman Fenton……….”Interesting. In fact, in EACH age category from 30 up the case rate is higher in the double vaccinated than the unvaccinated. Moreover, as we highlight here https://probabilityandlaw.blogspot.com/2021/10/comparing-all-cause-mortality-rate-by.html… ONS may be underestimating number of unvaccinated so unvacc rates are likely even lower than stated”
Also….
Dr Lamborghini Queuejump
@mcarrock
·
21 Oct
Replying to @profnfenton
I still want to see an official explanation for this yet none is forthcoming. There has been some handwaving from the FT about problems relating to NIMS vs ONS datasets, but I find these unconvincing – separately collected Scottish data points to same problem in same cohorts.
Follow the money.
Anti_socialist.
I added some information that you might find interesting to your post mentioning Microsoft in todays Roundup section.
Is the ‘Roundup’ as in Monsanto/Bayer?
I’ll get me coat.
The reason they are getting in a panic is that the data chime perfectly with the lived experience of everyone in the country. It is the vaccinated who are catching covid in their droves and, increasingly, it is the vaccinated who are ending up in hospital and sadlydying from Covid (although obviously, now, they all have significant comorbidities!?!) The Emperor hasn’t got any clothes on!!!
Excellent point. however, a correction is needed: “it is the vaccinated who are ending up in hospital and sadly dying within 28 days of a ‘positive’ PCR test.” It’s important, as ever, that we get the language right.
Yes, and in the context of that “language correction” it may be worth considering that a lot of the vaxxed people dying are ( as usual ) actually dying of non-covid things, **but** are being classified as covid cases precisely because of the test, *which is detecting the spike proteins produced as a result of the vaccinations*.
Others may know better, but I thought that the PCR test was ‘finding’ other pieces rather than spike pieces.
Would be good to know though, especially if the LFTs are using antibodies that stick to parts of the spike protein.
Single gene positives are normally counted as PCR positives, with the exception that testing positive for solely the S protein under PCR doesn’t count as a positive as you say. So you are right there.
Apparently this depends on the make of PCR test and/or lab doing the processing, some count as positive only if detect two of the usual 3 markers, others count as positive even if they only detect one of them. I did have an article from a science journal about this but I have no idea where my bookmark for it is anymore, sorry.
Like it;
’sadlydying’
to go with
’thescience’ and ‘thevaccine’
This issue first showed in the Zoe data in July, which was then “adjusted”, but it has now been a consistent trend in the data since August.
It can no longer be hidden anyway, as everyone knows someone who has been vaccinated and got COVID. I currently know of a number personally. So they won’t succeed in hiding it.
When the Zoe app was got at, it was an early indication that they knew the narrative was falling apart. I know many don’t agree but I think this helps Johnson deal with the criticism that “we locked down too late”. If he leaves cases to fall without interventions he can suggest that the lockdowns, which were “forced upon him”, were actually a damaging mistake. He can chuck Cummings and Gove under a bus in the process.
Looks like a spade, smells like a spade, must be a spade. Same can be said for these novel pharmaceutical products… Call something it’s not for long enough, people, however esteemed, will be brainwashed into believing it must do what the terminology says it must… Unless you change the definition of said word ‘vaccine’.
Sorry to repeat, but this explanation by Del Bigtree on the Pandemic Podcast is really excellent and explains what likely awaits the jabbed. If I were jabbed I would be seriously worried.
https://odysee.com/@pandemicpodcast:c/delbigtree:4
It appears to me that, at the risk of undermining the rest of the market, the manufacturers have gone for the term “vaccine”, rather than something else – lets say “mitigation drug”, because it gets around the complex test/trial protocol for novel drugs, and the use of “emergency use authorisation” is a bonus.
Here’s the data in chart form. I think it shows a trend.
Those look suspiciously like exponential rises week on week.
It’s not exponential as infection rates are coming down, but it may be that infection rates are coming down faster amongst those not vaxxed.
I meant that the curves for each age range appear exponential.
Despite all this there are a surprising number of people who still firmly believe that the vaccines stop you getting covid.
Do we similar charts for people in hospital and people dying?
Just to explain my chart above. It shows the apparent relative likelihood of someone vaxxed getting covid (or testing positive) compared to the unvaxxed. If the bar is below the ‘0’ line then it means that in that age group (the 30-39s, for instance during weeks 36 to 40 & the over 80s in week 36 & 37) the unvaxxed were more likely to get covid than the vaxxed. In each age group the picture has changed quite dramatically over the 7 weeks with the vaxxed now, in most age ranges being about 100% more likely to test positive.
Whatever the absolute truth is regarding the numbers they’ve been collated each week using the same methodology so the trend is certainly right.
“getting Covid” is two stages away from “testing positive”. It is amazing that this conflation is still going on after 20 months.
A acquaintance reports that despite his double jab and wearing a mask constantly whilst out, he caught Covid in a barber’s and suffered really badly from it, claiming that the vaccination likely saved him from dying.
Is that the sort of protection the gov promised us last January.
That’s “learning to live with covid” right there!
I’m a heretic for saying this: natural immunity is the only way out. I genuinely believe (personal view) that vaccines have bought us time but they are in no way a long term solution. The population needs gradually weening off them!
I agree in general. One of my sons, my wife & I all unvaxxed, all recently had the thing. 36 hours of mild headache, a week of a mild cough, aching back, that was it. My son has since had a nasty cold which made him far, far worse. But, the point was raised here last week from a report in the weekly surveillance report that people who’ve been jabbed, then get covid, aren’t developing ‘N’ type antibodies which may hinder the immune system fighting the thing in the future. This may, I guess, mean regular bouts of the thing. If this comes about, avoiding the vaccine & getting covid (with a 99.9% survival rate, for someone without comorbidities, as near as dammit 100% survival) will prove to have been the wisest option, whether you’re 70 or 7.
Indeed.
‘original antigenic sin’ ensures that people vaxinated with the original spike will respond to a newly mutated spike by producing the original antibodies – which will not be as efficient at counteracting the mutation, or may not counteract it at all.
Should have let it rip once they got over turning carehomes into death traps at the start.
The only way out of what?
My thoughts exactly. Out of what?
Delegitimisising all the lockdown and associated bollocks.
You’re not a heretic – it’s f.ing obvious.
“vaccines have bought us time“
“Bought us time” how? And where?
What would have happened if the “vaccines” had not existed, that would justify this spurious emergency and massive panic response?
Why haven’t communities like the Amish who largely avoided panicking and the “vaccines” and mostly caught the disease, suffered some kind of population catastrophe?
The US press tried to make out that the Amish had/would suffer a catastrophe as they let Covid rip through and some got sick, salivated over it as they did with some Jewish groups in NYC, then moved on when it didn’t happen.
Going back a year or so, wearing a mask is more likely to make you ill if you breath in a bit of Covid because it will not only prevent you from exhaling properly, the Covid will turn your mask into a comfy little petri dish right in front of your mouth.
Not unless you are coughing up living epithelial cells for the virus to infect. But it will provide a nice warm moist place for countless species of bacteria and other nasties to breed – ending up as comorbidities on your death certificate (if the rules haven’t been changed)
Agreed, should have said, exhaled bits of Covid will find in the mask a nice warm damp petri dish in which to breed alongside any other lurgies you should have been able to get rid of naturally.
The virus can only “breed”, replicate, if you are coughing up epithelial cells for it to replicate in. It can not “breed”/replicate in a place that doesn’t contain that very specific type of cells, however nice and moist and warm
Maybe it was the haircut that saved him from dying? Did he think of that?
I have to say over the last couple of weeks, a lot of this seems to be getting very worn at the edges. Stories seem increasingly desperate to fuel the narrative.
For the first time in a while a BBC HYS was actually against additional restrictions. The PM has admitted that having the vaccine in no way prevents transmission. That alone completely eradicates the need for vax passports….
‘Alex Berenson, a US journalist now banned from Twitter’.
The Covid cult Excommunication.
Banned for noting the lack of mortality benefit in the Pfizer study. Lol.
The world is now run by vaccine fundamentalists. They’ve captured the media and the tech companies.
PS anyone seen the latest YouGov poll?!
Apparently 1 in 3 want the rule of 6 for indoors.
I don’t know a single person including covidians who wants these rules!
Who has time to complete yougov studies apart from unemployed hermit mistanthropes?
Is that the very YouGov that was started and owned by non other than our favourite vaccine zealot, The Rt Hon Nadhim Zahawi and his wife. Funny that.
Nadhim Zahawi. Chairman of the shadowy Le Cercle 2015-2018.
https://en.wikipedia.org/wiki/Le_Cercle
Agenda since 1979:
All very above board and democratic.
And this is the man in charge of our children’s education now.
It is terrifying that so many people are still so terrified that they still feel this way. This hoo-haa has shown just how many people’s lives operate at a very childlike level. Their responses and attitudes are uninformed and infantile, Harry Potter was supposed to be children’s fantasy not a recipe for how adults should run their lives; being terrified of monsters and believing in magic potions.
That’s 2 out of 3 that don’t.
You know things are bad for them if they can’t even get a majority on their dodgy polls.
Like the made up vast majority of over 70s who supposedly want outdoor masks introduced yet quite obviously they are not doing so themselves.
And 3 in 9 want the rule of 666.
Perhaps the Professor needs to Halt Speigeling.
Admiring his own image?
It’s important, whether it’s above the line or down here in the comments, that we continue to trash the views of ‘experts’ like Spiegelhalter.
He was sometimes quite good at challenging Jeremy Vine when I listened to him last year.
Yes – he’s a mixed bag with certain biases.
The ‘percentage vaccinated’ figures produced by the gov used a different population estimate — for a long while that showed that for some age ranges more people had been vaccinated than existed in the country (I think 60-70 peaked at about 102% of the population).
The government provides us with data that ‘looks accurate’ but it is all smoke and mirrors.
IN this particular case it might be that the HSE is using a population estimate that’s too high — but the effect remains even with rather extreme reductions in the population estimate, and many actually organisations actually estimate the population to be higher (eg, based on food sales, amount of sewage produced, etc). Ie, it is possible that the vaccines are performing even worse.
I’d note that there are other sources that show vaccine effectiveness below zero, such as the recent paper on vaccine performance in Qatar.
Loads of double/triple jabbed f*ckwits I know have tested ‘positive’. Funnily enough, when you don’t believe in Covid, and never get tested, Covid never catches up with you at all.
As a double jabbed f*ckwit* several times compulsory tested as hospital inpatient, never been positive despite being immunocompromised thus being due a third primary jab on top of one & two and then a booster jab so four in all just for starters although the health service seem somewhat confused about implementing this.
Not had a cold or flu as far back as I can remember either.
*not through fear of Covid or belief in the efficacy of phoney vaccines rather not wishing to be discomforted at a later stage. Unnecessary as it turned out.
Odd that, isn’t it!
It’s almost as if Covid ‘case numbers’ rely on large numbers of people who have no symptoms, which in previous times would not have counted as ‘cases’ of any infection…
The old saying, “you are entitled to your own opinion, but not to your own facts” comes to mind.
I still back vaccination for adults 30+ (not sure about boosters and won’t get mine). I also totally back those who have seen the data on bad reactions, know that there is less than a year of data and say, “no thanks.” Clearly Mr. Whipple does not.
There is a pretty clear reason behind this. The vast majority of 30 plus unvaccinated have been infected. Yes, the greater percentage of real Covid deaths are among unvaccinated (and so the least healthy have sadly died), but the rest of the population they now have a stronger immunity base than those jabbed, and it hasn’t waned as much (still today, true double infections in people whose first was symptomatic is exceedingly rare).
why can’t we just allow people all the data and to make free choices?
Right, because some people want to remake society in their own image.
30+?
Why.what happens at 30 years of age that means that metric alone determines your need for a vaccine? Please include harms from this medical treatment in your assessment
I could understand backing the jab for the over 70s and for those whose immune systems aren’t all that, but why for over 30s, especially once waning immunity is considered and you’re against, what one can only logically conclude, is never ending rounds of ‘boosters’?
Simple answer: at 30 or 31 the risk of death from the vaccine becomes less then risk of death from Covid. I’m working with the best data I have at this point (how many deaths from the vaccine…yeah, that is hard to find).
You are right that truthfully only those 70+ and immuno compromised should have been encouraged to be jabbed and then leave it open to others. I got jabbed (age 50 at the time) because a) we were told get jabbed or lockdowns forever and b) the NHS ruled me immuno compromised. News to me but, I guess 500+ kidney stones (no, really) makes me such.
As more data comes out of vaccine issues, that line will rise to older and older. I’m just trying to base it on death vs death. Do I honestly think a 45 year old in good health should get jabbed? Um, no. But that is their decision to make.
But basic answer was the crossing point of fatality age risk.
Given that the long-term risks are unknown, that’s a very shaky claim. The decision is actually between a known very small risk from catching the virus, and an unknown risk (which could be large if ADE proves to be an issue) from the ‘vaccine’.
How do you do these calculations?
I based mine (age 48, female, BMI 21, good overall health) on http://www.qcovid.org risk of death in 3 month pandemic period of 1 in 55,000.
Vs risk of death from vaccine: seems to be at least 1 in 30,000. Quite possibly it is 1 in 10,000. Eudravigilance data suggests it is around that level.
I think a 3 month window is fine to use, as the vaccines also only have a benefit for around a 3 month window, as far as I can tell. Conveniently.
Maybe my BMI is the big differentiator? That needs to be considered.
(ETA also I now have COVID, so I know my risk of death from it unless I suddenly keel over, is actually zero. Though I’d better avoid walking under a bus in the next 22 days, as otherwise I could still be a covid death I guess).
I’d forgotten about the qcovid calculator, but it’s a good time to bring that back up. There were old conversations where we tried to do back of the envelope calculations to relate the risk figure from that calculator with the possible risk reduction that an experimental vaccine might provide in terms of assessing estimated benefits against estimated harms. Someone who has already had natural infection has I’d argue a lower risk than the calculator suggests. Talking of natural infection are you fully recovered now by the way? And then there was the issue that a theoretically effective vaccine that stopped you testing positive for covid if hospitalised for another condition but did not prevent your death from that other condition needed to be deducted from the qcovid risk in terms of calculating a potential vaccine benefit. But there was always an issue, how do you compare the risk of dying from covid in the 3 months around April 2020 with the future risk of dying from covid that a theoretically relatively safe and long term effective vaccine might prevent. Of course it was around March/April 2020 where people were getting ill from the symptoms of covid (albeit that this strongly… Read more »
“at 30 or 31 the risk of death from the vaccine becomes less then risk of death from Covid.”
Irrelevant.
What is relevant is the absolute risk reduction – which is less than minimal.
“I could understand backing the jab for the over 70s”
As one of those old farts – I can’t. Age doesn’t equal senility, and you have to be ga-ga to accept a jab on present evidence, with no controlled testing.
How do you know the majority of 30+ unvaccinated have been infected? The N protein prevalence data suggests 20pct of the population have been infected, and that will be be primarily in those who are either unvaccinated or were infected, then vaccinated. I don’t think you can tell who?
We know it’s not the vaccinated and then infected though.
The exact same population estimates used in the ‘cases’ table of the vaccine surveillance reports are also used in the hospitalised (after emergency care) and deaths tables to determine the rates per 100,000. Will’s articles have much more caveats about the ‘cases’ figures than the hospitalisations and deaths. And yet the supposed efficacy against hospitalisation and death may be because the unvaccinated proportion is understated. So he can hardly be called a purveyor of mis-information etc. The key to me is not whether the total population figures are right or not it is whether the proportion of unvaccinated vs double experimentally vaccinated is correct. In the 70-79 age group, if we take out the partially vaccinated, then of the remaining population of either unvaccinated or double ‘vaccinated’, the figures assume 95% of the age 70-79 age group is double ‘vaccinated’, and 5% unvaccinated. Given that there is twice the rate of ‘cases’ in that 70-79 age group in the double ‘vaccinated’ group, the true proportion of unvaccinated in the 70-79 group would need to be about 97.5% in order that the ‘case’ rate is the same in the vaccinated and double ‘vaccinated’. Is Spiegelhater really claiming that more than 97.5%… Read more »
For anyone who wants complementary data sets that show the UKHSA are reflecting what is seen elsewhere in the UK, you can see here.
https://www.health-ni.gov.uk/publications/vaccination-status-deaths-and-hospitalisations-previous-publications
https://www.health-ni.gov.uk/publications/vaccination-status-deaths-and-hospitalisations
This is data for Northern Ireland. In particular look to deaths by vaccination status (table 2). All adults.
Partially vaccinated (12.4 per 100,000) + fully vaccinated (11.7 per 100,000) = 24.1
Unvaccinated = 20 per 100,000
**Yes 24.1 v 20 for all adults.**
They should always be aggregating these partially and fully vaccinated groups in my view but they split them into two categories and many people will miss it.
I am even then still not happy with the definitions, but there you go.
Finally, the data there lines up with Public Health England data – as in around 75% of deaths in September for NI (the 4th deadliest month of the pandemic with 80% adults vaccinated).
I’m not sure it’s valid to add those two numerators together. They are for different groups. For example, if you were saying 10 per 100,000 men and 10 per 100,000 women then that doesn’t equal 20 per 100,000 people.
What it does tell us though is that the difference between one clotshot and two is statistically negligible. This means either the second clotshot is unnecessary as it has little benefit, or the unvaccinated stats are fraudulent.
Most people seem totally unable to grasp the concept of real levels of risk.
Good point. I glimpsed at it earlier and came to the same conclusion that you couldn’t add the two figures together.
It’s a good question, but actually – you can add them together because they are normalised. eg, if 1 in 10 is green and 5 in 10 are blue, then 6 in 10 are either blue or green. That is what BEPOP… was saying. You cannot simply add the raw figures and then normalise, but by using the same denominator, they are comparable. Or to to use the example above, if 50,000 out of 100,000 are women, and 50,000 out of 100,000 are men, then 50,000 + 50,000 out of 100,000 are either men or women.
Oops – on reflection I think my comment above is incorrect as they are different populations.
Does any of the stats take into account the number of school children using orange juice to get a positive result and bunk off school?
My son says he knows two kids who swore Sprite did it for them. Why waste perfectly good orange juice.
I’ve got a load of those lateral flow test things. My mother in law pushed them on us when our daughter got a cold, for some reason. They’ve just been sitting there, gathering dust. I’ll put them to good, scientific use, and report back.
Having looked through some of the published papers on vaccine side effects I found one that said the Pfizer version was safe. Fortunately authors have to declare any sponsorship of the research, for this paper the listed sponsors included Pfizer and the Gates foundation.
I came across something similar a few years ago when looking at the side effects of statins, there was one paper that said they didn’t cause raised blood sugar or muscle aches. That paper was sponsored by the manufacturer of one of the main statins used in this country.
If ever I look at any literature that says there’s no evidence of a problem when others say there may be, then I always check the affiliations of the author(s). Always be cynical and sceptical.
All this data shows is the government mandated experimental injections cause a significant increase in the risk of illness and death from the disease the injections are claimed to immunize. I don’t see what all the fuss is about.
The time for Professor David Spiegelhalter to have made his argument about ‘artefacts’ was surely when such comparisons first appeared. Of course, he didn’t squeal earlier because it suited him not too, since in many age groups the vaccine was then showing a marginal benefit.
But as has been pointed out before, it makes little difference if the unvaccinated denominator (for the rate calculation) has a degree of uncertainty. Put error bars of +/- 50% on the unvaccinated rate if you wish and the story stays the same: there is no statistically significant benefit to vaccination.
It is astonishing that Professor David Spiegelhalter thinks otherwise when studies from various countries, including Israel and Qatar, show the very same phenomenon, as did the cohort in the Pfizer trials who were vaccinated last year, and as Pfizer admitted to the FDA on September 17 that their vaccine effectiveness against infection was ‘not statistically significantly different from zero’.
Perhaps Professor David Spiegelhalter should turn his fire on Pfizer for that rare flash of honesty (there was an ulterior motive, though: to have boosters approved because the vaccine effectiveness was shot after a few months).
Quite. Also Scotland data (although that seems as shonky as the rest).
‘Artefacts’ on the part of the UKHSA versus ‘arty facts’ presented by our elected government and their MSM running-dogs.
Like the climate charlatans, these people run a mile from real world evidence, maintaining that only the models can be trusted.