New Lancet Study Confirms Plummeting Vaccine Effectiveness
A study appeared in the Lancet this week confirming that vaccine effectiveness against infection is fading fast.
The study involved 3,436,957 people over the age of 12 who are members of the healthcare organisation Kaiser Permanente Southern California. It sought to assess the effectiveness of the Pfizer vaccine against SARS-CoV-2 infections and COVID-19-related hospital admissions for up to six months, with a study period covering December 14th, 2020, to August 8th, 2021.
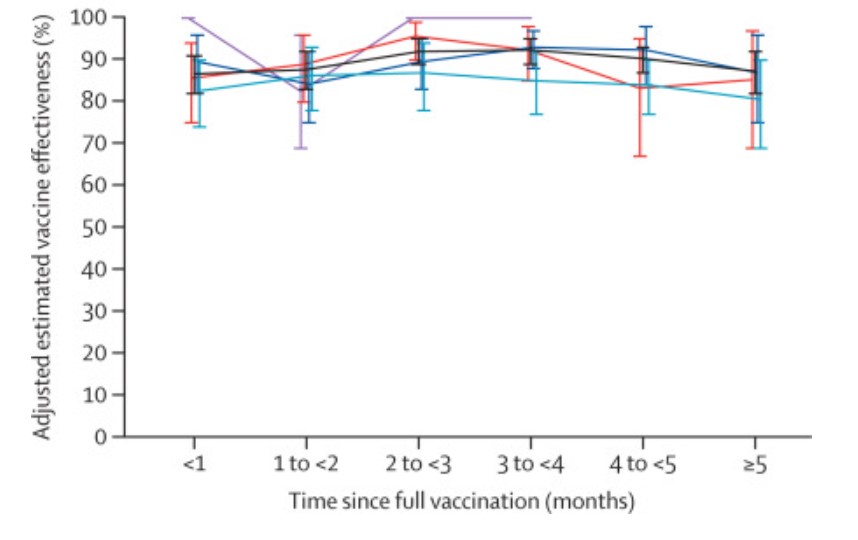
Comparing fully vaccinated to unvaccinated, and controlling for confounders such as prior infection, the researchers found that effectiveness against infection plummeted from 88% (95% confidence interval 86-89%) during the first month after double-vaccination to 47% (43-51%) after five months. The variation by age (depicted above) was largely within the margins of error.
Among sequenced infections, the researchers found vaccine effectiveness against Delta infection was 93% (85-97%) during the first month after double-vaccination but dropped to 53% (39-65%) after four months. Effectiveness against infection from other variants the first month after double-vaccination was 97% (95-99%), but declined to 67% (45-80%) at 4-5 months.
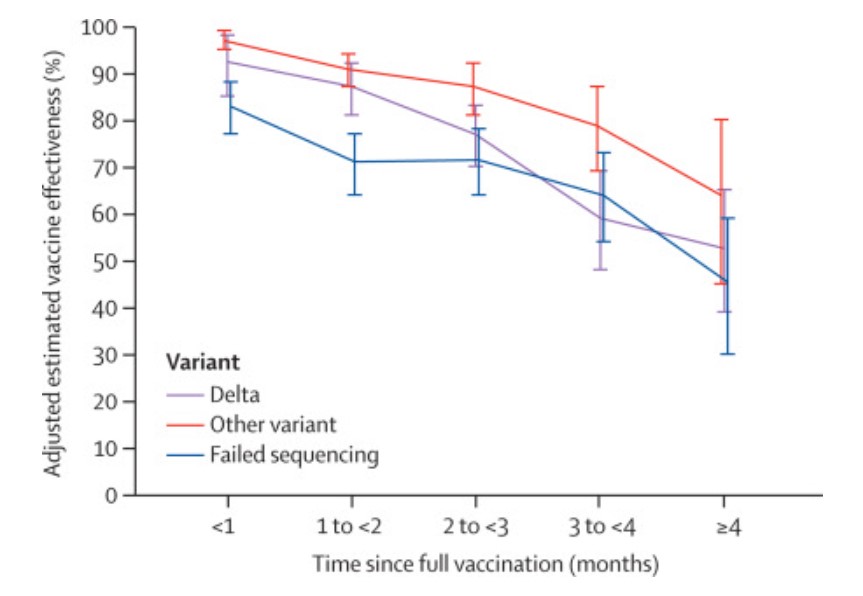
Vaccine effectiveness against hospital admissions for Delta infection held up at around 93% (84-96%) for the six months across all ages.
However, the researchers note that the latest data from Israel “suggests that some reduction in effectiveness against hospital admissions has been observed among older people (65 years and over) roughly six months after receiving the second dose of [Pfizer]”.
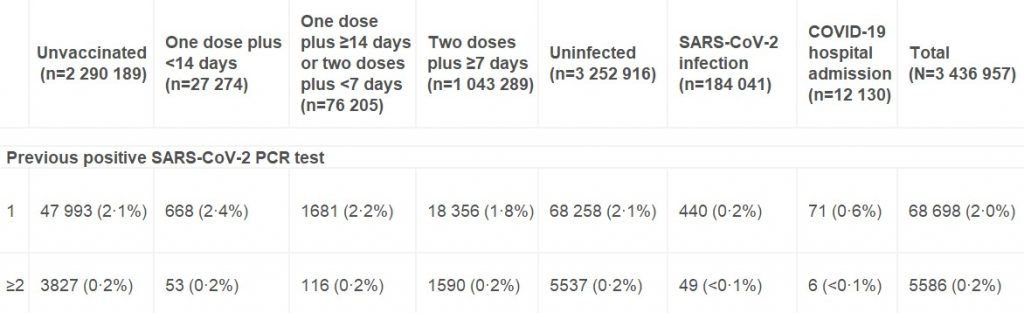
One question that’s arisen recently is to what extent vaccine effectiveness estimates are affected by whether more people who have been previously infected decide not to be vaccinated. According to this study the answer is: not very much at all. Among the unvaccinated, 2.3% had one or more previous positive PCR tests, only slightly more than the 2% of the double-vaccinated who did.
It’s also worth noting that although this study adjusts its raw estimates for no fewer than 22 potential confounding variables, the adjusted figures differ very little from the unadjusted figures in almost all cases. This suggests that unadjusted estimates from large population samples are often a fair approximation in the absence of sophisticated statistical analysis.
Given that the adjusted figures were little different to the unadjusted figures, however, it’s not immediately clear why the vaccine effectiveness estimates in this study, while low and declining, are so much higher than the latest unadjusted estimates derived from Public Health England data (namely, negative vaccine effectiveness in the over-40s, including minus-66% in those in their 40s). It doesn’t appear to be merely a matter of additional time elapsing, as most people in the U.K. weren’t double vaccinated until April, May or June, meaning only four or five months have elapsed until September, the same time period as in the study.
Could it be because the study period ended on August 8th, when the Delta surge in California was just getting going (see below)?
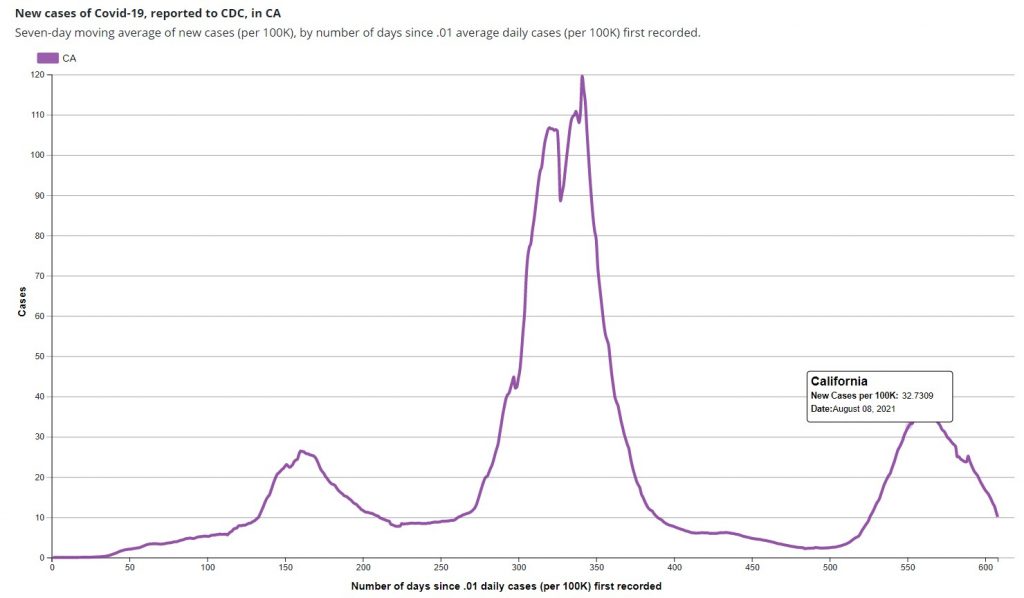
In the U.K. the vaccine effectiveness didn’t plunge until the second half of the Delta surge, the first part being dominated by infections in the unvaccinated (for reasons still not entirely clear). Did the new study finish too early to see the dramatic effect we’ve seen in England?
The authors say their study indicates that the decline in vaccine effectiveness is primarily a function of time rather than variant-related. However, the evidence from England would suggest otherwise, as in the same period of time, but later in the Delta surge, the decline has been far greater.
The decline in vaccine effectiveness in England was confirmed last week in a new Government-funded study (not yet peer-reviewed), which found that the reduction in transmission “declined over time since second vaccination, for Delta reaching similar levels to unvaccinated individuals by 12 weeks for [the AstraZeneca vaccine] and attenuating substantially for [Pfizer]”. In other words, within just three months AstraZeneca did nothing to prevent transmission, and Pfizer was scarcely better.
One of the main recommendations of the authors of both studies in light of their findings is for regular booster jabs – in the case of the first, where many of the authors are employees of and investors in Pfizer, this may be deemed hardly surprising. However, if effectiveness against serious disease is holding up, why give people boosters just to stop them getting and spreading what is effectively a cold, and which bestows more robust immunity as it goes? Furthermore, if the effectiveness declines after as little as three months, is it even possible to deliver enough boosters to have any impact on infection and transmission? Would it not be much better to say that the vaccines, by offering personal protection from serious disease to those who want it, have done their job? Better to move on and abandon any ideas of vaccine passports and mandates and boosters, and in general the now almost wholly pointless obsession with Covid vaccines.
To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
You can look at this in two ways, depending which hat you’re wearing: either they weren’t very effective in the first place (and you’ll never be able to prove otherwise unless you had a time machine) or this is a way of pushing boo$ter shot$ (yes, that was intentional).
I’m looking at it a third way: The fake vaccine made absolutely no difference and the stats above are in line with the seasonal change of summer to autumn. People generally start getting colds and flu this time of year onwards.
The roll out of the fake vaccine was perfectly timed to make it look effective but only for a certain period of time. They’ll use this to argue that everyone needs a ‘booster’ which will again have absolutely no positive effect on the recipient. When the deaths start ratcheting up during winter, they’ll argue it is the fault of the “anti-vaxxers” and they’ll introduce the vaxport.
But how do we account for the 4 to 10x worse covid ‘cases’/deaths in 2021 vs 20? Something has very clearly worsened as far as covid goes, and the people who are trying to make it look *better* are also in charge of the reporting.
The vaccines account for the increased “Covid” deaths over the summer of 2021 compared to last year. The vaccines are guilty until proven innocent, which won’t happen. Watch out for a new death surge as the “boosters” are rolled out on the still sleeping masses.
The hike in ‘cases’ has been due to schools testing children and the reintroduction of crowds at sporting events.
Deaths, see Rowan’s reply. I would add to it the ongoing use of Midazolam to give pensioners a “good death” since the start of this scam.
Midazolam Matt killed your granny
Completely agree . . . said the same myself before that they came out at the right time – you could roll that out into the ‘first place’ option that they weren’t effective but take your point. Flu season is coming and then of thousands will die and the NHS will be at ‘breaking point’ – like they do every year but people have short memories and like to gaslight.
The crux of the matter is people are stupid – not everyone, but seemingly a large majority, even those that appear to be informed and intelligent just because they have letters after their name or Dr.
Correct. Masks did nothing, lockdown did nothing, “vaccines” did nothing. Virus did what virus gonna do.
A key issue I have with these studies is that they do not take into account those who have been killed by the vaccine itself. They always exclude people who die shortly after having the vaccine, which results in the vaccine appearing to be more effective than it is. In the case of the first wave of older people, this could be as much as 30k people. You just have to look at the large peak post first vaccine roll-out to see this. If you take a population and challenge it in this way, killing off the most vulnerable, the remaining population will appear to be more resistant to the same challenge if exposed to it again, but this is only because the more vulnerable have been removed. This alone could entirely explain the apparent effectiveness of the vaccine reducing hospitalisations and deaths while not reducing infections and also explains why the apparent effectiveness only lasts 6 months because by then more of the remaining population enter the more vulnerable group.
Someone please prove me wrong.
You won’t be proved wrong. It’s as clear as day, that the vaccines were never meant to prevent or treat Covid, whatever it actually is. While the “vaccines” are a cash cow, their real purpose is depopulation. Watch out for an immediate surge in “Covid” deaths as the boosters are rolled out.
Yes. France had quite a lot less “vaccinations” than the UK over January to July before Manual Chevron started his vax apartheid thing, and yet the UK had more total “Covid” deaths reported.
This just in: wearing garlic around your neck does not necessarily provide complete protection against vampires.
This is how I always think of idiot mask-wearers. Wearing a mask in supermarkets etc and saying “Look, I’ve not caught Covid. They work!” is as ridiculous as wearing a crucifix around your neck and declaring, “Look, I’ve not been attacked by any evil spirits. It works!” It’s literally an emotional support talisman and theatre at the end of the day.
That’s only one of the two main reasons for wearing a face-nappy – the other is of course virtue signalling: “look, aren’t I a caring person!”.
The absence of any calls to improve these vaccines in effectiveness at preventing spread of disease, preventing illness or in terms of side effects, coupled with a clamour to roll out ‘boosters’ suggests that this entire episode has nothing to do with health outcomes and everything to do with a vaccine ID.
They will soon transmogrify into a social credit system and eventually become the vehicle behind central bank digital currency. We shall soon live beneath the eyes of a global digital panopticon, the Davos set want to impose feudalism and the left somehow think this is a good idea.
This has gone from “crazy conspiracy theory” to “most likely explanation” really fast, hasn’t it?
Th “vaccines” have everything to do with health outcomes, though not in any good way. Of course control is part of the equation, you absolutely need it when you are in the process of murdering 95% of the population.
Do they at least claim that this boilerplate non-sequitur was written by an AI?
The absence of improved vaccines (claims about them being available now being made last year) suggests that the original product is still selling good enough, hence, more R&D expenses are not justified. And that’s about it.
We’re also technically living in a feudal society where the state grants fiefdoms to private operators for commercial exploitation, eg railways, utilities, health service, prison operation, $younameit. They should resurrect feuds as well. That would be more fun.
If you add in the higher infection rate after the first jab and them fraudulently counting these infections, illnesses, hospitalisations and deaths as those of the unvaccinated, it’s a wash.
At best.
Absolutely. There’s fairly good evidence of a period of enhanced protection against covid in months 2-4/5 (approx) which they have conveniently carved out to rig the vaccinated cohort, but I would not be surprised one bit if the net effect of the vaccine is well into the negative.
There is no evidence or little chance of the “vaccines” providing any protection from Covid or from anything else, for that matter. There were far fewer problems in the summer of 2020 with no “vaccines” than in the summer of 2021.
I think at this stage no one cares… They’ve been sold the lie that vaccines are the answer and that’s that. We know it’s all bullshit
They will care before too long.
Behind closed doors, governments will be reacting to the reality that there is no way to vaccinate your way out of this. That’s assuming, charitably, that they had a good-faith expectation to the contrary from the outset.
As I see it, this is *the* crossroads. Governments can either press on, risking that the case against vaccines become more obvious, the whole thing blowing up in their faces; alternatively, they may well take this opportunity to extend the offer of natural immunity certificates in the vaccine passport.
This latter is the worst possible outcome, IMO, because it will persuade some sceptics that this is not all bad, they’re being reasonable, nothing more to resist here.
Natural immunity certificates = covid parties.
Let Ferguson loose as to how long his computer says it would take for the whole population to become immune, sorry, infected.
Brilliant idea, almost embracing the concept of natural immunity – and that would never do.
Even the sheep might smell a rat.
Vaccinate our way out of what? The coofs are just another endemic disease now. Still infectious, like influenza. Still potentially fatal, like influenza. Our NHS is not collapsing any more than it ever does – except by forcing staff who have long, long since build natural immunity to not show up. Excess mortality is not up significantly (or is actually down).
“Vaccine passports” have nothing to do with immunity. They are about begging the State for – revocable – permission to live our daily lives. There is no other explanation for pushing ahead with them, reasonable or otherwise.
This latter is the worst possible outcome, IMO, because it will persuade some sceptics that this is not all bad, they’re being reasonable, nothing more to resist here.
That may not be the worst possible outcome, yes there’s always disability and death. I have to wonder just why anyone would think health passports are a good idea and just who the heck is voting up such nonsense. You trolls are really out in force today.
I know this was in the past so it’s now memory holed, BUT…
Wasn’t 50% the minimum effectiveness to be worthwhile in a jab?
Look at the Declaration of Interests. This “study” was produced by academic shills on the Big Pharma payrol. It is a sales pitch dressed up as an academic study. The forgone conclusion was always going to be that we need more injections. What a joke. Funny how a previous Lancet study done by people NOT on the Big Pharma payroll concluded that the injections have ZERO efficacy.
The ‘study’ authors are “are employees of and hold stock and stock options in Pfizer”.
That should have been in the intro.
Zero efficacy for immunity and transmission, but effective for genocide.
Well lets hope that there waning effectiveness means they wont do the long term harm some predict, only time will tell on that one.
Quick first glance through the article and there it is, ‘regular booster jabs’. Totally agree with the last sentence. But Wales have agreed with the Segregation passports
If this jab is not stimulating a proper immune response then it is not, by definition, a vaccine. So not only is it potentially life threatening, it isn’t even effective.
Thought the manufacturer’s said from the start that this does not give immunity
Agreed.
But the problem is that naive Boris went on and on about how the vaccines were going to be the cavalry coming over the hill to save us, the silver bullet etc. People not surprisingly assumed that the jabs would give them full immunity.
There should be a silver bullet for Johnson and his cronies!
Yep; it is a dangerous, and not very effective, therapeutic.
My understanding of this is that the mRNA drug presents our immune system with a single spike protein identified as part of Covid 19. So, as the virus mutates (and not much!) the immune system lacks the necessary reference and the ‘vaccine immunity’ wanes (or vanishes). This is primary school predictable, not some unforeseen, devilish property of a never seen before virus. Which begs the question, why use this method? Why are all the ‘vaccines’ mRNA, a new technology? Why was the traditional approach completely ignored?
oh and surprise!
The spike protein causes clots!
And of course the spike protein is found on the virus.
but not in the pure form from the AZ or the runaway form in the mRNA jab
What do you mean “pure” and “runaway”?
But the spike protein manufactured in your cells after mRNA highjacking isn’t the same as that in the circulating virus.
Specifically there are changes to the codons in the mRNA to make manufacture ‘easier’ (read cheaper) and the effects of changes from the viral spike to the mRNA manufactured spike were never specifically tested. There are also changes in the mRNA sequence to ensure that the immune system is specifically bypassed to maximise the longevity of the mRNA while it manufactures the ‘new’ spike protein.
Why are all the ‘vaccines’ mRNA, a new technology? Why was the traditional approach completely ignored?
The Pfizer and Moderna vaccines are the only ones that use mRNA. All the others (AZ, Johnson and Johnson in the UK – but others worldwide) use different techniques.
You can’t get the AZ direct clot-shot anymore (or is it if you’re under 40, despite the unrare side effects being the same).
Quite agree BUT when everyone trundled along to the “jab fest” they had no idea which jab they were having.
The AZ one is a usual vaccine format with side effects and the mRNA ones are experimental also with side effects.
If you’re healthy it’s a lose lose situation.
AstraZeneca, Johnson and Johnson and the Russian one are also not traditional vaccines. They’re not the mrna style but they’re also designed to produce this spike protein which is causing all the problems.
Yes it is the protein which may or may not be causing problems. This has two interesting consequences:
The protein is also found on the virus (that’s the whole point of producing it) which may explain why getting Covid is rather more likely to give you a blood clot than being vaccinated (both risks are very small)
mRNA as a mechanism for producing the protein is no more risky than any other method. Robert Malone has no more credentials for assessing the safety of the vaccine than any other doctor (not that he ever invented a vaccine in his life).
Dr. Robert Malone is a medical doctor and an infectious-disease researcher, and is recognized as the discoverer of in-vitro and in-vivo RNA transfection and the inventor of mRNA vaccines while he was at the Salk Institute in 1988. His research was continued at Vical in 1989, where the first in-vivo mammalian experiments were designed by him. Between 1988 and 1989, the doctor wrote the patent disclosures for mRNA vaccines and therefore does have the “credentials for assessing the safety of the vaccine”.
But, as Stevey points out, it is the protein that has the potential to cause problems, not the method of producing it. So Malone’s expertise in mRNA technology is irrelevant.
So why on this earth, knowing what we all know for certain now as opposed to 20 months ago, would you think it beneficial to inject yourself with a preparation, all the ingredients of which remain undisclosed to this day ( FDA FoI request pending via ICAN in the US) that induces your body to produce “trillions” of Alpha variant S1 spike proteins to produce an immunological response to “kill” said proteins and thus avoid CV19, when SARS COV2, a GoF edited chimera as admitted by its inventors, mutates just as all known viruses do.
Or have I missed the fact that these jabs have been modified to deal with the Delta variant/mutation – or even “pan” variants of SARS COV2? Because if you know that to be the case, they don’t appear to be working, do they?
“So Malone’s expertise in mRNA technology is irrelevant.”
Bit like saying that Nils Bohr’s expertise was as a nuclear physicist; nuclear fission has the potential to cause harm , so Bohr’s expertise in nuclear fission is irrelevant.
“Trillions” referenced to recent “SARS COV2 cautionary” blog post by Dr M Kendrick
You need to bury your confirmation bias and get your basic facts right, you prat!
We all need to try our hardest to bury our confirmation bias.
“The protein is also found on the virus (that’s the whole point of producing it) which may explain why getting Covid is rather more likely to give you a blood clot than being vaccinated (both risks are very small)” If that is your conclusion from you experience as a pathologist doing post mortems it would have some validity. However, medics worldwide have expressed deep concern at the incidence of clotting throughout the body of affected patients, as well as the unknown long term risks thereof, eg Myocarditis. The risk is only small if it does not immediately impact YOUR health – if however you ARE adversely affected, say with any form of inflammatory condition such as Myocarditis, I suggest the risk is enormous, up front and very personal; in your clinical experience, how do your patients recover from Myocarditis as just one of the manifestations of the inflammatory effects of these mRNA jabs? “mRNA as a mechanism for producing the protein is no more risky than any other method” Please enlighten us all be comparing the adverse effects as reported via VAERS /UK Yellow Card between the mRNA and non mRNA jabs – genuinely I don’t know, and wish to… Read more »
“Yes it is the protein which may or may not be causing problems. This has two interesting consequences”
What else could be causing the inflammatory effect in jabbed individuals? Has there not been a study comparing the effects of SARS COV2 injected into trial subjects, one cohort with the S1 spike protein and one without?
I seem to remember that the study found that the cohort without the S1 spike protein did not become infected with CV19, whilst the cohort that did have the jab including the S1 spike protein DID contract CV19?
As you know , I am no scientist and rely on them for information; this would appear to be …conclusive… as far as the Alpha variant goes ( at the very least?) As all Coronaviruses are >80% genetically similar ( ref Dr MY et al) what would your logic tell you?
The AZ vaccine is a usual vaccine format as in the flu shots people have been having for years as it uses the same ChAdOx1 technology.
However, as you rightly say they do produce the spike protein and that is why even as a 65 year old I have refused all vaccines for the past 40 years.
BUT when everyone trundled along to the “jab fest” they had no idea which jab they were having
It was made very clear to my wife and myself. I haven’t asked anyone else!
They had no choice in the matter, they were told which one they were having when they arrived there. If they wanted the AZ one and not an mRNA one they had no choice.
COVID JABS are ALL GENE THERAPY and they are ALL EXPERIMENTAL. Confirmed in this document by the pioneer of the technology, Robert Malone MD Bioethics of Experimental COVID Vaccine Deployment under EUA: It’s time we stop and look at what’s going down. https://www.rwmalonemd.com/news/xjz6sws8let4yt39ddsgs3leessg8d “I believe that adult citizens must be allowed free will, the freedom to choose. This is particularly true in the case of clinical research. These mRNA and recombinant adenovirus vaccine products remain experimental at this time. Furthermore, we are supposed to be doing rigorous, fact-based science and medicine. If rigorous and transparent evaluation of vaccine reactogenicity and treatment-emergent post-vaccination adverse events is not done, we (the public health, clinical research and vaccine developer communities) play right into the hands of anti-vaxxer memes and validate many of their arguments. The suppression of information, discussion, and outright censorship concerning these current COVID vaccines which are based on gene therapy technologies cast a bad light on the entire vaccine enterprise. It is my opinion that the adult public can handle information and open discussion. Furthermore, we must fully disclose any and all risks associated with these experimental research products. In this context, the adult public are basically research subjects that are not… Read more »
“The Pfizer and Moderna vaccines are the only ones that use mRNA” I think it politic to point out that what you dont say is that the mRNA jabs – because as we know even Pfizer does not deem them vaccines ( ref Dr D Martin, Pfizer EUA application to FDA, Pfizer describe them as “gene editing therapy:) – only involve the inducement within your body to produce an immunological response to the S1 spike protein of the Alpha variant and ignores all other antigens of the same variant; how else would you explain the increasing prevalence of (?Delta? variant ) infections within the jabbed vs unjabbed – i.e the experience in Israel, very widely reported, and happening elsewhere? With respect, may I suggest you read Omar Khan’s piece “It Was Always a Con: The COVID Debacle” – illuminating. The conclusion I draw is that the jabs do have a beneficial effect in reducing the most severe effects of infected people, ie similar to early treatment protocols devised by medics worldwide and that work, but do not stop infection, and have little or no effect on transmission. COST of the jabs – many many many billions of GBP/EUs/$ that could… Read more »
All the ‘vaccines’ aren’t mRNA but the ones that have been EUA’d in the UK and USA (other countries are available) are.
Interestingly the non-mRNA vaccines that have been developed are having great difficulty getting EUAs through the MHRA EMA and FDA – funny that, its not that they aren’t owned by Pfizer Moderna’s (owners the CDC FDA scientists and administrators) or anything like that is it?
Another interesting point is that the contamination of mRNA vaccines being delivered in Japan has lead to the Japanese medicine agency junking them and buying large number of doses (and presumably EUAing ) of the non-mRNA Novavax vaccine. Watch that space to see if controlling the number of spike proteins circulating after jabbing significantly reduces the adverse events widely reported for the mRNA vaccines.
All the ‘vaccines’ aren’t mRNA but the ones that have been EUA’d in the UK and USA (other countries are available) are.
I am afraid that is not true. AZ and Johnson and Johnson have been EUA’d in the UK and the USA and neither is mRNA based.
It hasn’t been ignored Valneva is a covid vaccine using traditional technology – it is a true vaccine. It is made in Scotland and France.
Buuuuut not available in the UK due to ‘supply chain problems’ as cited by MHRA.
Because the virus has not been isolated.
I think it was Naomi Wolf who said Moderna’s presentation to investors from the beginning stated that their vaccines are designed to require regular boosters, thus producing an ongoing revenue stream for investors.
https://www.cnbc.com/2018/04/11/goldman-asks-is-curing-patients-a-sustainable-business-model.html
Goldman Sachs asks in biotech research report: ‘Is curing patients a sustainable business model?’
Is allowing fake banks to stay open sustainable?
In a way, this might be good news for the jabbed……..does waining effectiveness mean that the ‘pointless poison’ is leaving the system? Therefore reducing the likelihood of ADE infection?
Very convenient results for the ‘vax’ makers! Come in Nos xxxxxxx, your time is up: booster-time again!
81% of Covid-19 deaths are among the Vaccinated, Male Teen Deaths have rised by 63% since they were offered the jab, Covid-19 Deaths are 12 times higher than this time last year – https://theexpose.uk/2021/10/05/uk-has-fallen-81-percent-covid-deaths-vaccinated-teen-deaths-63-percent-higher/
These so called vaccines are no better than the gamma globulin injections us medics used to get 30 years ago for needle sticks that potentially infected us with hepatitis B before a proper hepatitis vaccine existed. Antibodies were extracted from previously infected people and injected into the recipient. It was not termed vaccination. It was a short term treatment to protect against infection. The covid vaccines are not vaccines at all. They are innoculations, hence the need for repeated boosters. A vaccine confers protection from infection – or at least it did until they changed the definition. Gamma globulin therapy was safer as it did not rely on gene therapy that hijacks the immune system to produce a toxic antigen to stimulate antibody production.
This ‘study’ by Pfizer employees and shareholders used data supplied by Kaiser Permanente – which is a WEF partner. The CEO of KP is Greg Adams – who is a WEF ‘Governor and Steward’. The WEF is driving the Great Reset/4th Industrial Revolution.
This ‘study’ used data supplied by Kaiser Permanente – which is a WEF partner. The CEO of KP is Greg Adams – who is a WEF ‘Governor and Steward’. The WEF is driving the Great Reset/4th Industrial Revolution.
So… when you say that “Vaccine effectiveness against hospital admissions for Delta infection held up at around 93%”… what exactly are we using as a control here? The models who assume the Earth’s population will be wiped out over night? Or the unvaccinated population?
This is like saying the road drives the car.
A vaccine stimulates the immune system by imitating a natural infection. It does not create the immune response itself.
This is basic stuff that seems to be ignored everywhere.
and the COVID jabs are like protecting from a road by having a million copies of the white paint in the middle.
Glad Will pointed to the funders of the Kaiser Permanente organisation. It’s essentially a rubber stamping factory of vaccine safety. Their recent study on adverse reactions reported something like 30 cases in 6.5m individuals (they use Vaccine Data Link not VAERS) and declared that every one of them was just noise and expected.
https://jamanetwork.com/journals/jama/fullarticle/2784015
I think it especially interesting that they adjust for 22 factors in this vaccine efficacy study in the Lancet. They do similar kinds of multiple adjustments in the adverse reaction study.
I’ll speculate that the Lancet study has tried many ways to get the answer they wanted. And couldn’t. I’ll guess here that the efficacy numbers they’ve reported are in fact a lot worse.
I welcome the honestly with these reports, but surely all it means is it justifies the junta banging us all back up in our homes again ?
Only those who haven’t been triple vaxxed, surely? Yet STILL they fall for it.
This is for Pfizer, I guess. Would be interesting to know the equivalent numbers for AZ.
“Time since full vaccination” is only part of the picture. What about all the periods between the first shot and ‘full vaccination’?
Immunological blood workup from double vaxxed shows a compromised immune system. Elevated granulocytes, decreased lymphocytes and natural killer cells, all indicative of auto immune disorder.
This entire sickening rhetoric is only psychological propaganda to promote regular “boosters”.
But for a start, natural immunity is always better than any vaccine [althought the C19 jab isn’t a vaccine], and second C19 doesn’t exist, therefore all rest are LIES, distractions.
Effectiveness for a month? With all the adverse events cdc VAERS, you have to ask yourself, is it worth taking the experimental biologicals, still in trial, with no lying term safety or efficacy. How could so many people be bamboozled? A worrying development are all the young people suffering serious cardiac conditions post vaxx. Sweden has suspended Moderna now, due to this adverse event.
The vaxxed are now the majority suffering from Covid, some have become seriously ill and hospitalised. No long term safety or efficacy data, but daily things are looking dire for the vaxxed. See CDC VAERS and all European and UK health data.
I fear you are correct.
From a formerly duped x2 jabbed, but no longer duped “Very concerned of…..address redacted”
Natural Immunity has ALWAYS been more effective than any snake oil poison, all through history. Not ONE vax has had a control group study included (for a reason). Even this pointless, unnecessary garbage has had the token control group sabotaged by giving the placebo group the real Mccoy within months, thus eliminating the chance to collect meaningful data……………….For example UK Measles mortality was about 1,250 per million in 1900, and by the time the widespread vax programme came in during the early 60s it was lower than 5 per million. So clean water, sanitation, better housing and the ability to store food longer was the real reason for the drop in mortality, yet the Big Pharma cash cow snake oils took all the credit